A ten-year-old boy with bubonic plague was taken to the hospital in the Kosh-Agach district of the Altai Republic, reports lenta.ru.
The child was admitted to the infectious diseases department of the district hospital on July 12 with a temperature of about 40 degrees. He is currently in moderate condition. “Specialists found out that he had contact with 17 people, six of whom were children. All of them are placed in isolation and are under observation. So far, they have shown no signs of infection,” the hospital noted.
Health workers suggested that the boy could have contracted the plague while camping in the mountains. It is noted that in the region the disease was recorded in marmots.
Bubonic plague is an infectious disease that has claimed more human lives throughout history than all other diseases combined. Despite all the advances in medicine, it is impossible to completely get rid of the plague, since the causative agent of the disease - the bacterium Yersinia pestis - lives in natural reservoirs, where it infects its main carriers - marmots, gophers and other rodents. These reservoirs exist all over the world and it is unrealistic to destroy them all.
OpenClipart-Vectors, 2013Therefore, about three thousand cases of bubonic plague are registered annually in the world, and outbreaks occur even in highly developed countries. Thus, in October 2015, it was reported that a teenage girl from Oregon in the USA was infected with bubonic plague.
However, in countries with underdeveloped healthcare systems, plague outbreaks occur much more often and lead to greater casualties. Thus, in 2014, an outbreak of bubonic plague was registered in Madagascar, which killed 40 people.
In August 2013, doctors confirmed a case of bubonic plague in Kyrgyzstan: 15-year-old Temirbek Isakunov contracted the dangerous disease after he and his friends ate marmot kebab.
 The marmot is a carrier of plague. PublicDomainPictures, 2010
The marmot is a carrier of plague. PublicDomainPictures, 2010 She commented on this incident on her blog:
The media begins to noisily discuss the possible consequences of the cases of bubonic plague that have appeared in Kyrgyzstan, or more precisely, in how many days will it begin in our country from the Kyrgyz who came to us and cough on us. In this regard, let me remind you that:
1. The danger of the appearance of plague on the territory of Russia is constant, since the plague is a zoonosis, that is, a disease the main reservoir of which is animals. These are gophers and a number of other species living in deserts, semi-deserts, steppes, etc. There are more than a thousand permanent plague foci on the territory of Russia, and there are also a lot of foci in the republics of the former USSR and other neighbors of Russia.
2. The main methods for controlling plague are as follows:
A) Limiting the number of natural hosts (poisoning gophers),
B) Vaccination of those who have to work in these outbreaks,
B) Border control of those entering (people and animals)
3. Human diseases of the plague are inevitable for countries with outbreaks. In Russia, the plague causes about one death per year; in the USA, as far as I remember, about 10 die per year.
4. Plague is a particularly dangerous disease due to its high mortality rate. If it is detected, emergency anti-epidemic measures are taken. The plague has a very bad reputation, since in medieval Europe one third of the population died from its epidemics. However, among infectious diseases it now accounts for only a small proportion of deaths. Malaria accounts for the largest number of deaths (more than a million per year).
5. Methods of combating the plague epidemic are very simple. They identify the sick person, drag him into quarantine and treat him, at the same time they grab and drag into quarantine everyone with whom he has been in contact for the last few days. If one of those people gets sick, they seize and isolate those with whom he was in contact. So, in the conditions of a state that is organized enough to carry out such a thing, outbreaks are nipped in the bud.
6. An interesting feature of the plague is that there is one pathogen, but two diseases: pneumonic plague and bubonic plague. The form of development of the disease depends on where the pathogen enters: into the blood or into the lungs.
7. If the pathogen enters the lungs, pneumonic plague develops. It progresses as a rapidly developing acute respiratory infection, followed by hemoptysis and death. From the moment of infection to the first pronounced symptoms - about a day, until death - about 3. Mortality - 100%. It can be successfully treated with some modern antibiotics, but only if treatment is not started too late. Therefore, in the case of pneumonic plague, the outcome depends on the timeliness of hospitalization and the start of treatment, and literally minutes count.
 The causative agent of plague is Yersinia pestis. Larry Stauffer, 2002
The causative agent of plague is Yersinia pestis. Larry Stauffer, 2002 8. If the pathogen enters the bloodstream, bubonic plague develops - a severe blood fever with a mortality rate (in the absence of antibiotic treatment) of about 50%. The duration of the disease from infection to recovery or death is about a couple of weeks. It got its name from the characteristic giant enlargement of the axillary lymph nodes to formations similar in size and shape to a bunch of grapes.
9. The two indicated forms of plague with the same pathogen are associated with a transmission option. With pneumonic plague, the patient sneezes and coughs, droplets of saliva containing the pathogen scatter and infect others, getting into the lungs. In bubonic plague, the carrier is blood-sucking insects: fleas, lice, etc. People are often infected through bloodsuckers from mice and rats suffering from the plague. By the way, plague epidemics in medieval Europe were also associated with the fact that there were a lot of brown rats. In recent years they have been replaced by another species, white and larger, which is less susceptible to plague.
In principle, it is possible for the plague to transition during epidemics from the bubonic to the pneumonic form and back, but due to these features, epidemics usually occur either only as bubonic, or only as pneumonic.
There is a third, more exotic form of plague - intestinal, when the pathogen enters the stomach, but for this you have to go to India, to the sacred waters of the Ganges...
10. If a plague patient is identified (including a deceased person), due to the above, fun begins, accompanied by panic: platoons of police with machine guns that surround the building with identified contacts, and serious people in anti-plague suits with flamethrowers, scared to death of them (joke).. Over the past 50 years, there have been several (about three) cases of detection of plague being brought into Moscow and several false panics.
11. There is no need to be more scared than usual by people who cough and sneeze. Spraying nearby eastern people with insect repellents from spray cans is the same.
It could be worse
In addition to the plague, outbreaks of an even more dangerous disease - anthrax - are regularly recorded in the vastness of our homeland. The source of this infection is domestic animals: cattle, sheep, goats, pigs. Infection can occur when caring for sick animals, slaughtering livestock, processing meat, as well as through contact with animal products (hides, skins, fur products, wool, bristles) contaminated with spores of the anthrax microbe.
Infection can also occur through soil in which spores of the anthrax pathogen persist for many years. Spores enter the skin through microtraumas; When contaminated foods are consumed, an intestinal form occurs. The high lethality of the pulmonary and intestinal forms, as well as the ability of the pathogen spores to remain viable for many years, are the reason for the use of the anthrax bacillus as a biological weapon.
 William Rafti, 2003
William Rafti, 2003 The largest epidemic of this disease occurred in 1979 in Sverdlovsk. Since then, small outbreaks of this disease have occurred regularly. Thus, in August 2012, an outbreak of anthrax with fatal cases was recorded in the Altai Territory - in the village of Marushka and the village of Druzhba.
In August 2010, an anthrax outbreak was recorded in the Tyukalinsky district of the Omsk region. The epidemic began with the death of horses on a private farm, which the owners did not report. The dead animals were not even properly buried. As a result, at least six people fell ill, at least one of whom, 49-year-old Alexander Lopatin, died.
In addition, rumors of smallpox cases regularly arise, although the World Health Organization has officially declared the disease eradicated. However, rumors, as a rule, are not confirmed, and one of the last outbreaks of smallpox was recorded in Moscow in the fifties of the last century. He talks about her:
I got vaccinated today at clinic 13 (it was moved from Neglinnaya to Trubnaya St., 19с1, by the way, a long time ago). While they were waiting for the sister, the doctor, an elderly but cheerful, clear-eyed aunt, told a story about the smallpox epidemic in Moscow in the 50s.
I found it on Wiki and am posting it here:
In the winter of 1959 we found ourselves in a bad situation. Moscow artist Kokorekin visited India. He happened to be present at the burning of a deceased Brahmin. Having gained impressions and gifts for his mistress and wife, he returned to Moscow a day earlier than his wife was waiting for him. He spent this day with his mistress, to whom he gave gifts and in whose arms he spent the night, not without pleasure. Having timed the plane's arrival from Delhi, he arrived home the next day. After giving the gifts to his wife, he felt bad, his temperature rose, his wife called an ambulance and he was taken to the infectious diseases department of the Botkin Hospital.
 A girl infected with smallpox (Bangladesh). James Hicks, 1975
A girl infected with smallpox (Bangladesh). James Hicks, 1975 The senior surgeon on duty, Alexey Akimovich Vasiliev, in whose team I was on duty that day, was called for a consultation in the infectious diseases department with Kokorekin, regarding the imposition of a tracheostomy on him due to breathing problems. Vasilyev, having examined the patient, decided that there was no need to apply a tracheostomy and went to the emergency room. By morning the patient became ill and died.
The pathologist who performed the autopsy invited the head of the department, Academician Nikolai Aleksandrovich Kraevsky, into the dissecting room. An old pathologist from Leningrad came to visit Nikolai Alexandrovich and was invited to the dissecting table. The old man looked at the corpse and said, “Yes, my friend, variola vera is black smallpox.” The old man was right.
They reported to Shabanov. The machine of Soviet health care began to spin. They imposed a quarantine on the infectious diseases department, and the KGB began tracing Kokorekin’s contacts. The story of his early arrival in Moscow and a night of bliss with his mistress came to light. As it turned out, the wife and mistress behaved in the same way - both ran to thrift stores to hand over gifts. There were several cases of smallpox in Moscow, which ended in death. The hospital was quarantined, and it was decided to vaccinate the entire population of Moscow with smallpox vaccine.
There was no vaccine in Moscow, but there was one in the Far East. The weather was bad and no planes were flying. Finally the vaccine arrived and vaccinations began. I suffered it very hard, I did not have immunity against smallpox, although I was vaccinated in 1952, when an epidemic of smallpox began in Tajikistan, brought from Afghanistan in the traditional way - carpets were thrown across the border on which patients with smallpox lay.
Update: I found the details here. It turns out that the ill-fated Kokorekin was present not only at the burning of the Brahmin, who definitely died of smallpox, but also the Brahmin’s hut. And I thought - how did he manage to get infected, how? After all, before burning the body is wrapped in several layers of cloth, and the high temperature of the fire should have killed all the vibrios. But vibrio is “resistant to environmental influences, especially to drying and low temperatures. It can persist for a long time, for a number of months, in crusts and scales taken from pockmarks on the skin of patients” (wiki). In that hut there were millions of flakes of skin and dust with vibrios - that’s how I became infected.
And it was after this incident and thanks to the USSR that they adopted a program to eradicate smallpox throughout the world. In the wild forests of India, tribes were shown photographs of people suffering from smallpox. So they got rid of it!
More than half of the population of Europe in the Middle Ages (XIV century) was wiped out by a plague known as the Black Death. The horror of these epidemics remained in the memory of people after several centuries and was even captured in the paintings of artists. Then the plague repeatedly visited Europe and claimed human lives, albeit not in such quantities.
Currently, the plague remains a disease. About 2 thousand people become infected annually. Most of them die. Most cases of infection are observed in the northern regions of China and Central Asian countries. According to experts, there are no reasons or conditions for the emergence of black death today.
The causative agent of the plague was discovered in 1894. Studying epidemics of the disease, Russian scientists developed principles for the development of the disease, its diagnosis and treatment, and an anti-plague vaccine was created.
Symptoms of plague depend on the form of the disease. When the lungs are affected, patients become highly contagious, as the infection spreads into the environment through airborne droplets. With the bubonic form of plague, patients are slightly contagious or not contagious at all. There are no pathogens in the secretions of the affected lymph nodes, or there are very few of them.
Treatment of plague has become much more effective with the advent of modern antibacterial drugs. Mortality from the plague has since dropped to 70%.
Plague prevention includes a number of measures to limit the spread of infection.
Plague is an acute infectious zoonotic vector-borne disease, which in the CIS countries, together with diseases such as cholera, tularemia and smallpox, is considered (OOI).
Rice. 1. Painting “The Triumph of Death”. Pieter Bruegel.
Plague agent
In 1878, G. N. Minkh and in 1894, A. Yersin and S. Kitazato, independently discovered the causative agent of the plague. Subsequently, Russian scientists studied the mechanism of development of the disease, the principles of diagnosis and treatment, and created an anti-plague vaccine.
- The causative agent of the disease (Yersinia pestis) is a bipolar, non-motile coccobacillus, which has a delicate capsule and never forms spores. The ability to form a capsule and antiphagocytic mucus does not allow macrophages and leukocytes to actively fight the pathogen, as a result of which it quickly multiplies in the organs and tissues of humans and animals, spreading through the bloodstream and through the lymphatic tract throughout the body.
- Plague pathogens produce exotoxins and endotoxins. Exo- and endotoxins are contained in the bodies and capsules of bacteria.
- Bacterial aggression enzymes (hyaluronidase, coagulase, fibrinolysin, hemolysin) facilitate their penetration into the body. The stick is able to penetrate even intact skin.
- In the ground, the plague bacillus does not lose its viability for up to several months. It survives in the corpses of animals and rodents for up to one month.
- The bacteria are resistant to low temperatures and freezing.
- Plague pathogens are sensitive to high temperatures, acidic environment and sunlight, which kill them in only 2 - 3 hours.
- Pathogens are stored in pus for up to 30 days, in milk for up to 3 months, and in water for up to 50 days.
- Disinfectants destroy the plague bacillus in a few minutes.
- Plague pathogens cause disease in 250 animal species. Among them, the majority are rodents. Camels, foxes, cats and other animals are susceptible to the disease.
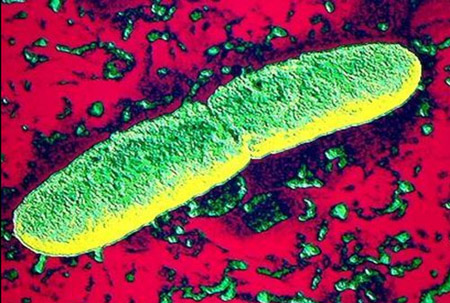
Rice. 2. In the photo, the plague bacillus is the bacterium that causes the plague - Yersinia pestis.
Rice. 3. The photo shows the causative agents of the plague. The intensity of coloration with aniline dyes is greatest at the poles of bacteria.
Php?post=4145&action=edit#
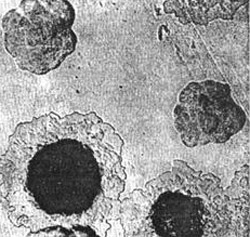
Rice. 4. In the photo, the pathogens of the plague are growing on a dense colony medium. At first, the colonies look like broken glass. Next, their central part becomes denser, and the periphery resembles lace.
Epidemiology
Reservoir of infection
Rodents (tarbagans, marmots, gerbils, gophers, rats and house mice) and animals (camels, cats, foxes, hares, hedgehogs, etc.) are easily susceptible to the plague bacillus. Among laboratory animals, white mice, guinea pigs, rabbits and monkeys are susceptible to infection.
Dogs never get plague, but they transmit the pathogen through the bites of blood-sucking insects - fleas. An animal that dies from a disease ceases to be a source of infection. If rodents infected with plague bacilli hibernate, their disease becomes latent, and after hibernation they again become distributors of pathogens. In total, there are up to 250 species of animals that are sick, and therefore are a source and reservoir of infection.

Rice. 5. Rodents are the reservoir and source of the plague pathogen.

Rice. 6. The photo shows signs of plague in rodents: enlarged lymph nodes and multiple hemorrhages under the skin.

Rice. 7. In the photo, the small jerboa is a carrier of the plague in Central Asia.

Rice. 8. In the photo, the black rat is a carrier not only of plague, but also of leptospirosis, leishmaniasis, salmonellosis, trichinosis, etc.
Routes of infection
- The main route of transmission of pathogens is through flea bites (transmissible route).
- The infection can enter the human body when working with sick animals: slaughter, skinning and cutting (contact route).
- Pathogens can enter the human body with contaminated food products as a result of their insufficient heat treatment.
- From a patient with pneumonic plague, the infection spreads through airborne droplets.

Rice. 9. The photo shows a flea on human skin.

Rice. 10. The photo shows the moment of a flea bite.

Rice. 11. The moment of a flea bite.
Pathogen carriers
- The carriers of pathogens are fleas (in nature there are more than 100 species of these arthropod insects),
- Some types of ticks are carriers of pathogens.

Rice. 12. In the photo, the flea is the main carrier of the plague. There are more than 100 species of these insects in nature.

Rice. 13. In the photo, the gopher flea is the main carrier of plague.
How does infection occur?
Infection occurs through an insect bite and rubbing of its feces and intestinal contents when regurgitating during feeding. When bacteria multiply in the intestinal tube of a flea under the influence of coagulase (an enzyme secreted by pathogens), a “plug” is formed that prevents human blood from entering its body. As a result, the flea regurgitates a clot onto the skin of the bitten person. Infected fleas remain highly infective for 7 weeks to 1 year.

Rice. 14. In the photo, the appearance of a flea bite is pulicotic irritation.

Rice. 15. The photo shows a characteristic series of flea bites.

Rice. 16. View of the lower leg with flea bites.

Rice. 17. Appearance of the thigh with flea bites.
Man as a source of infection
- When the lungs are affected, patients become highly contagious. The infection spreads into the environment through airborne droplets.
- With the bubonic form of plague, patients are slightly contagious or not contagious at all. There are no pathogens in the secretions of the affected lymph nodes, or there are very few of them.
Mechanisms of plague development
The ability of the plague bacillus to form a capsule and antiphagocytic mucus does not allow macrophages and leukocytes to actively fight it, as a result of which the pathogen quickly multiplies in the organs and tissues of humans and animals.
- Plague pathogens penetrate through damaged skin and then through the lymphatic tract into the lymph nodes, which become inflamed and form conglomerates (buboes). Inflammation develops at the site of the insect bite.
- Penetration of the pathogen into the bloodstream and its massive reproduction leads to the development of bacterial sepsis.
- From a patient with pneumonic plague, the infection spreads through airborne droplets. The bacteria enter the alveoli and cause severe pneumonia.
- In response to the massive proliferation of bacteria, the patient’s body produces a huge number of inflammatory mediators. Developing disseminated intravascular coagulation syndrome(DIC syndrome), in which all internal organs are affected. Hemorrhages in the heart muscle and adrenal glands pose a particular danger to the body. The developed infectious-toxic shock causes the death of the patient.
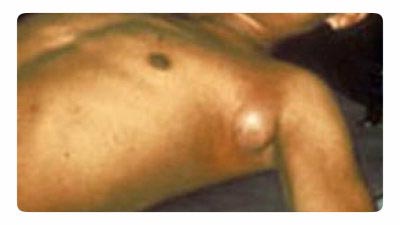
Rice. 18. The photo shows the bubonic plague. Typical enlargement of the lymph node in the axillary area.
Plague symptoms
The disease manifests itself after the pathogen enters the body on days 3–6 (rarely, but there have been cases of the disease manifesting itself on days 9). When infection enters the blood, the incubation period is several hours.
Clinical picture of the initial period
- Acute onset, high temperatures and chills.
- Myalgia (muscle pain).
- Excruciating thirst.
- A strong sign of weakness.
- Rapid development of psychomotor agitation (“crazy” patients are called). A mask of horror (“plague mask”) appears on the face. Lethargy and apathy are less common.
- The face becomes hyperemic and puffy.
- The tongue is thickly covered with a white coating (“chalky tongue”).
- Multiple hemorrhages appear on the skin.
- The heart rate increases significantly. Arrhythmia appears. Blood pressure drops.
- Breathing becomes shallow and rapid (tachypnea).
- The amount of urine excreted decreases sharply. Anuria develops (complete absence of urine output).

Rice. 19. In the photo, assistance to a plague patient is provided by doctors dressed in anti-plague suits.
Forms of plague
Local forms of the disease
Cutaneous form
At the site of a flea bite or contact with an infected animal, a papule appears on the skin, which quickly ulcerates. Next, a black scab and scar appear. Most often, skin manifestations are the first signs of more severe manifestations of the plague.
Bubonic form
The most common form of manifestation of the disease. Enlarged lymph nodes appear near the site of the insect bite (inguinal, axillary, cervical). More often one lymph node becomes inflamed, less often several. When several lymph nodes become inflamed at once, a painful bubo is formed. Initially, the lymph node has a hard consistency, painful on palpation. Gradually it softens, acquiring a dough-like consistency. Next, the lymph node either resolves or becomes ulcerated and sclerosed. From the affected lymph node, the infection can enter the bloodstream, with the subsequent development of bacterial sepsis. The acute phase of bubonic plague lasts about a week.

Rice. 20. The photo shows the affected cervical lymph nodes (buboes). Multiple hemorrhages of the skin.

Rice. 21. In the photo, the bubonic form of plague affects the cervical lymph nodes. Multiple hemorrhages in the skin.

Rice. 22. The photo shows the bubonic form of plague.
Common (generalized) forms
When the pathogen enters the bloodstream, widespread (generalized) forms of plague develop.
Primary septic form
If the infection, bypassing the lymph nodes, immediately enters the blood, then the primary septic form of the disease develops. Intoxication develops at lightning speed. With the massive proliferation of pathogens in the patient’s body, a huge number of inflammatory mediators are produced. This leads to the development of disseminated intravascular coagulation syndrome (DIC), which affects all internal organs. Hemorrhages in the heart muscle and adrenal glands pose a particular danger to the body. The developed infectious-toxic shock causes the death of the patient.
Secondary septic form of the disease
When the infection spreads beyond the affected lymph nodes and pathogens enter the bloodstream, infectious sepsis develops, which is manifested by a sharp deterioration in the patient’s condition, increased symptoms of intoxication and the development of DIC syndrome. The developed infectious-toxic shock causes the death of the patient.

Rice. 23. In the photo, the septic form of plague is the consequences of disseminated intravascular coagulation syndrome.

Rice. 24. In the photo, the septic form of plague is the consequences of disseminated intravascular coagulation syndrome.

Rice. 25. 59-year-old Paul Gaylord (resident of Portland, Oregon, USA). Plague bacteria entered his body from a stray cat. As a result of the development of a secondary septic form of the disease, his fingers and toes were amputated.

Rice. 26. Consequences of DIC syndrome.
Externally disseminated forms of the disease
Primary pulmonary form
The pneumonic form of plague is the most severe and dangerous form of the disease. The infection penetrates the alveoli through airborne droplets. Damage to the lung tissue is accompanied by cough and shortness of breath. An increase in body temperature occurs with severe chills. The sputum at the beginning of the disease is thick and transparent (vitreous), then it becomes liquid and foamy, mixed with blood. The scant data from physical examinations do not correspond to the severity of the disease. DIC syndrome develops. Internal organs are affected. Hemorrhages in the heart muscle and adrenal glands pose a particular danger to the body. The patient's death occurs from infectious-toxic shock.
When the lungs are affected, patients become highly contagious. They form around themselves a focus of a particularly dangerous infectious disease.
Secondary pulmonary form
It is an extremely dangerous and severe form of the disease. Pathogens penetrate into the lung tissue from affected lymph nodes or through the bloodstream during bacterial sepsis. The clinical picture and outcome of the disease are the same as in the primary pulmonary form.
Intestinal form
The existence of this form of the disease is considered controversial. It is assumed that infection occurs through the consumption of contaminated products. Initially, against the background of intoxication syndrome, abdominal pain and vomiting appear. Then comes diarrhea and numerous urges (tenesmus). The stool is copious, mucous-bloody.
Rice. 27. Photo of an anti-plague suit - special equipment for medical workers when eliminating the outbreak of a particularly dangerous infectious disease.
Laboratory diagnosis of plague
The basis for diagnosing plague is the rapid detection of the plague bacillus. First, bacterioscopy of smears is performed. Next, a culture of the pathogen is isolated, which infects experimental animals.
The material for research is the contents of the bubo, sputum, blood, feces, pieces of tissue from the organs of deceased animals and corpses.
Bacterioscopy
The causative agent of plague (Yersinia pestis) is a rod-shaped bipolar coccobacilli. Analysis for the detection of plague bacillus by direct bacterioscopy is the simplest and fastest method. The waiting time for the result is no more than 2 hours.
Crops of biological material
The culture of the plague pathogen is isolated in specialized high-security laboratories designed to work with. The growth time of the pathogen culture is two days. Next, an antibiotic sensitivity test is performed.
Serological methods
The use of serological methods makes it possible to determine the presence and growth of antibodies in the patient’s blood serum to the plague pathogen. The time to receive results is 7 days.

Rice. 28. Diagnosis of plague is carried out in special sensitive laboratories.
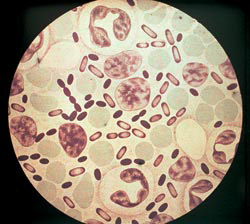
Rice. 29. The photo shows the causative agents of the plague. Fluorescence microscopy.

Rice. 30. The photo shows the culture of Yersinia pestis.
Immunity to plague
Antibodies against the introduction of the plague pathogen are formed quite late in the development of the disease. Immunity after an illness is not long-lasting or intense. There are repeated cases of the disease, which are as severe as the first.
Treatment of plague
Before treatment begins, the patient is hospitalized in a separate room. Medical personnel serving the patient wear a special anti-plague suit.
Antibacterial treatment
Antibacterial treatment begins at the first signs and manifestations of the disease. Among antibiotics, preference is given to antibacterial drugs of the aminoglycoside group (streptomycin), the tetracycline group (vibromycin, morphocycline), the fluoroquinolone group (ciprofloxacin), and the ansamycin group (rifampicin). An antibiotic of the amphenicol group (cortrimoxazole) has proven itself well in the treatment of the skin form of the disease. For septic forms of the disease, a combination of antibiotics is recommended. The course of antibacterial therapy is at least 7–10 days.
Treatment aimed at different stages of development of the pathological process
The goal of pathogenetic therapy is to reduce intoxication syndrome by removing toxins from the patient’s blood.
- The administration of fresh frozen plasma, protein drugs, rheopolyglucin and other drugs in combination with forced diuresis is indicated.
- Improved microcirculation is achieved by using trental in combination with salcoseryl or picamilon.
- If hemorrhages develop, plasma pheresis is immediately performed to relieve disseminated intravascular coagulation syndrome.
- If blood pressure drops, dopamide is prescribed. This condition indicates the generalization and development of sepsis.
Symptomatic treatment
Symptomatic treatment is aimed at suppressing and eliminating the manifestations (symptoms) of the plague and, as a result, alleviating the suffering of the patient. It is aimed at eliminating pain, cough, shortness of breath, suffocation, tachycardia, etc.
The patient is considered healthy if all symptoms of the disease have disappeared and 3 negative bacteriological test results have been obtained.
Anti-epidemic measures
Identification of a plague patient is a signal for immediate action, which includes:
- carrying out quarantine measures;
- immediate isolation of the patient and preventive antibacterial treatment of service personnel;
- disinfection at the source of the disease;
- vaccination of persons in contact with the patient.
After vaccination with an anti-plague vaccine, immunity lasts for a year. Re-vaccinate after 6 months. persons at risk of re-infection: shepherds, hunters, agricultural workers and employees of anti-plague institutions.

Rice. 31. In the photo, the medical team is dressed in anti-plague suits.
Disease prognosis
The prognosis of plague depends on the following factors:
- forms of the disease,
- timeliness of treatment started,
- availability of the entire arsenal of medicinal and non-medicinal treatments.
The most favorable prognosis is for patients with lymph node involvement. The mortality rate for this form of the disease reaches 5%. In the septic form of the disease, the mortality rate reaches 95%.
The plague is, and even with the use of all the necessary medications and manipulations, the disease often ends in the death of the patient. Plague pathogens constantly circulate in nature and cannot be completely destroyed and controlled. Symptoms of plague are varied and depend on the form of the disease. The bubonic form of plague is the most common.
Articles in the section "Particularly dangerous infections"Most Popular
Plague (“Black Death”, Pestis) is a particularly dangerous, acute, naturally focal zoonotic* bacterial infection, with multiple routes of transmission, and characterized by a feverish-intoxication syndrome, as well as predominant damage to the skin and lungs.
A brief historical sketch: without exaggeration, we can add the prefix “most” to the following characteristics - the oldest, most dangerous to this day, breaking records for the severity of the disease and the highest mortality rate, as well as for the level of contagiousness (infectiousness) - in all these points the plague has practically no equal .
The still completely illiterate natives passed on their everyday experience from generation to generation: when dead rats appeared in a hut, the entire tribe left the area, imposing a taboo and never returning.
The 3 largest plague pandemics have been recorded in the history of the world:
In the 3rd century there was the first description, in the territories where Libya, Syria, and Egypt are now located.
The pandemic in the 6th century in the Roman Empire until the end of Justinian’s reign is the “Justinian pandemic.” During this period, thanks to the accumulated experience, quarantine began to be introduced for 40 days in order to prevent the spread of infection.
Late 19th century - third pandemic, most common in seaports. Also, this century became a turning point, because during this period the causative agent of the plague itself was discovered by the French scientist Yersin in 1894.
Long before these pandemics, there were many epidemics that are countless... One of the largest was in France, in the 16th century, where one of the most famous psychics, doctors and astrologers lived - Nostradamus. He successfully fought the “Black Death” with the help of herbal medicine, and his recipe has survived to this day: sawdust of young cypress, Florentine iris, cloves, fragrant calamus and woody aloe - rose petals were mixed with all these components and “rose” tablets were made from this mixture pills." Unfortunately, Nostradamus was unable to save his wife and children from the plague...
Many cities where death reigned were burned, and local doctors, trying to help the infected, wore special anti-plague “armor”: a leather cloak to the very toes, a mask with a long nose - various herbs were placed in this nasal section and, when inhaled, heated air caused evaporation of antiseptic substances contained in herbs, the inhaled air was practically sterile. This mask was protected by crystal lenses, rags were stuck in the ears, and the mouth was rubbed with raw garlic.
It would seem that the era of “antibiotics” would forever eliminate the danger of the plague, they thought so for a short time, until the scientist Bacon modeled a genetic mutant of the plague - an antibiotic-resistant strain. Also, vigilance cannot be reduced because there have always been and are natural foci (territorially aggressive). Social upheaval and economic depression are predisposing factors in the spread of this infection.
The causative agent is Yersinia Pestis, it looks like an ovoid rod, G-, does not have spores or flagella, but forms a capsule in the body. On nutrient media it gives characteristic growth: on broth agar - plague stalactites, on solid media, the first 10 hours in the form of “broken glass”, after 18 hours in the form of “lace handkerchiefs”, and by 40 hours “adult colonies” are formed.

There are a number of structural characteristics that are components of pathogenicity factors:
Capsule – inhibits the activity of macrophages.
Pili (small villi) - inhibit phagocytosis and cause the penetration of the pathogen into macrophages.
Plasmocoagulase (also coagulase) - leads to plasma coagulation and disruption of the rheological properties of blood.
Neurominidase - ensures adhesion and attachment of the pathogen due to the release of its receptors on the surface.
The specific antigen pH6 is synthesized at a temperature of 36°C and has antiagocyte and cytotoxic activity.
Antigens W and V – ensure the reproduction of the pathogen inside macrophages.
Catalase activity provided by adenylate cyclase suppresses the oxidative burst in macrophages, which reduces their protective ability.
Aminopeptidases – provide proteolysis (cleavage) on the cell surface, inactivation of regulatory proteins and growth factors.
Pesticin is a biologically active component of Y.pestis that inhibits the growth of other representatives of the genus Yersinia (Yersiniosis).
Fibrinolysin - ensures the breakdown of the blood clot, which subsequently aggravates the clotting disorder.
Hyaluronidase - ensures the destruction of intercellular connections, which further facilitates its penetration into the underlying tissues.
Endogenous purines (the role of their presence is not completely clear, but upon breakdown they form uric acid, which is potentially toxic).
Endotoxin is a lipopolysaccharide complex that has toxic and allergenic effects.
Rapid growth at a temperature of 36.7-37°C - this feature, in combination with antiphaocytic factors (listed above), makes the growth and reproduction of the plague pathogen practically unimpeded.
The ability of the pathogen to sorb (accumulate/collect) hemin (derived from heme - the non-protein part of the Fe3+ transporter in the blood) - this property ensures the reproduction of the pathogen in tissues.
Mouse toxin (lethal = C-toxin) – has cardiotoxic (heart damage), hepatotoxic (liver damage) and capillary toxic effects (impairs vascular permeability and causes thrombocytopathies). This factor is manifested by a blockade of the transfer of electrolytes in mitochondria, i.e. blockade of the energy depot.
All pathogenicity (harmfulness) is controlled by genes (there are only 3 of them) - Bacon influenced them by modeling an antibiotic-resistant mutant of the plague and thus warned humanity about a moving threat in conditions of inappropriate and uncontrolled use of antibiotics.
Resistance of the plague pathogen:
Retains in sputum for 10 days;
On linen, clothes and household items stained with mucus - for weeks (90 days);
In water – 90 days;
In buried corpses - up to a year;
In open warm spaces – up to 2 months;
In bubo pus (enlarged lymph node) – 40 days;
In soil - 7 months;
Freezing and thawing, as well as low temperatures, have little effect on the pathogen;
The following are destructive: direct UV radiation and disinfectants cause instant death, at 60°C - death within 30 minutes, at 100°C - instantaneous death.
Plague refers to natural focal infections, that is, there are territorially dangerous zones in epidemic terms; there are 12 of them on the territory of the Russian Federation: in the North Caucasus, Kabardino-Balkaria, Dagestan, Transbaikalia, Tuva, Altai, Kalmykia, Siberia and the Astrakhan region . Globally, natural foci exist on all continents except Australia: Asia, Afghanistan, Mongolia, China, Africa and South America.
In addition to natural focal (natural) zones, synanthropic foci (anthropouric) are also distinguished - urban, port, ship.
Susceptibility is high, without gender or age restrictions.
Causes of plague infection
The source and reservoir (guardian) of infection are rodents, lagomorphs, camels, dogs, cats, sick people. The carrier is a flea, which remains infective for up to a year. The plague microbe multiplies in the digestive tube of fleas and in the front part of it forms a “plague block” - a plug of a huge amount of the pathogen. When bitten, with the reverse flow of blood, some of the bacteria are washed off from this plug - this is how infection occurs.
Routes of infection:
Transmissible (through flea bites);
Contact – through damaged skin and mucous membranes when skinning infected animals, during slaughter and cutting of carcasses, as well as through contact with biological fluids of a sick person;
Contact household – through household items contaminated with biological media of infected animals/humans;
Airborne (through the air, from a patient with pneumonic plague);
Nutritional – when eating contaminated foods.
Plague symptoms
The incubation period is considered from the moment of introduction of the pathogen to the first clinical manifestations; with plague, this period can last from several hours to 12 days. The pathogen more often penetrates through the affected skin or mucous membranes of the digestive/respiratory tract; it is captured by tissue macrophages, and part of the pathogen remains at the entrance gate, and part is transferred by macrophages to regional (nearby) lymph nodes. But as long as the pathogen dominates phagocytosis and suppresses its action, the body does not identify the pathogen as a foreign object. But phagocytosis is not completely suppressed, some of the pathogens die and after death, an exotoxin is released and upon reaching its threshold concentration, clinical manifestations begin.
The period of clinical manifestations always begins acutely, suddenly, with the first symptoms of intoxication in the form of chills, high fever >39°C lasting for 10 days and/or until death, severe weakness, body aches, thirst, nausea, vomiting; cyanotic, with dark circles under the eyes - these changes against the background of an expression of suffering and horror are called the “mask of plague.” The tongue is covered with a thick, white coating - “chalky tongue”. There is a standard pathogenetic symptom complex (that is, due to the specific mechanism of action of the pathogen, 4 standard symptoms are formed in varying degrees of manifestation):
At the site of the entrance gate, a primary focus is formed, which can undergo stages and stop at one of them: spot - papula - vesicle.
Enlargement of regional lymph nodes (formation of a “plague bubo”) to impressive sizes (≈apple) due to the multiplication of the pathogen in it and the formation of an inflammatory-edematous reaction. But it often happens that the process proceeds so quickly that death occurs even before the development of the plague bubo.
ITS (infectious-toxic shock) develops as a result of degranulation of neutrophils (NF) and the death of the pathogen with the release of endotoxin. It is characterized by a certain degree of manifestation and the main diagnostic criteria are: changes in the nervous system (state of consciousness) + or ↓t° of the body + hemorrhagic rash (pinpoint rashes in the oropharynx) + hemorrhages in the mucous membranes + peripheral circulatory disorders (coldness, pallor or blue discoloration of the extremities, nasolabial triangle, face) + changes in pulse and blood pressure (↓) + changes in intracranial pressure (↓) + the formation of renal failure, manifested as a decrease in daily diuresis + changes in acid-base balance (acid-base status) towards acidosis
DIC syndrome (disseminated intravascular coagulation) is a very serious condition, which is based on disorganization of the coagulation and anticoagulation systems. DIC occurs in parallel with the development of ITS and manifests itself ↓Tr +clotting time + ↓degree of clot contraction + positive procoagulation test.
Clinical forms of the disease:
Localized (cutaneous, bubonic);
generalized (pulmonary, septic).
The forms of the disease are indicated in the order in which the disease can develop in the absence of treatment.
Cutaneous form: tissue changes occur at the site of the entrance gate (one of 4 standard symptoms); in severe or fulminant cases, a phlyctena (blister) filled with serous-hemorrhagic contents, surrounded by an infiltrative zone with hyperemia and edema, may develop. When palpated, this formation is painful, and when opened, an ulcer forms with black necrosis (eschar) at the bottom - hence the name “black death”. This ulcer heals very slowly and always leaves scars after healing and, due to slow healing, secondary bacterial infections often form.
Bubonic form: “Plague bubo” is an enlarged lymph node, either one or several. The increase can be from the size of a walnut to an apple, the skin is shiny and red with a cyanotic tint, the consistency is dense, palpation is painful, it is not fused with the surrounding tissues, the boundaries are clear due to concomitant periadenitis (inflammation of the peri-lymphatic tissues), on the 4th day the bubo softens and fluctuation appears (a feeling of excitement or hesitation when tapping), on the 10th day this lymphatic focus is opened and a fistula with ulceration is formed. This form can lead to both secondary bacterial septic complications and septic plague complications (i.e. plague bacteremia) with the introduction of the plague pathogen into any organs and tissues.
Septic form: characterized by the rapid development of INS and DIC syndrome, multiple hemorrhages on the skin and mucous membranes come to the fore, and bleeding begins in the internal organs. This form can be primary - when a massive dose of the pathogen is ingested, and secondary - when there are secondary bacterial complications.
Pulmonary form the most dangerous in an epidemiological sense. The onset is acute, as in any other form; pulmonary symptoms (due to the melting of the walls of the alveoli) join the 4 standard clinical symptoms and come to the fore: a dry cough appears, which after 1-2 days becomes productive - the sputum is initially foamy, glassy , clear and consistency like water, and then becomes purely bloody, with countless amounts of excitability. This form, like the septic one, can be either primary - with aerogenic infections, or secondary - a complication of the other forms listed above.
Diagnosis of plague
1. Analysis of clinical and epidemiological data: in addition to standard clinical manifestations, the place of residence or current location is examined and whether this place corresponds to a natural outbreak.
2. Laboratory criteria:
- UAC: Lts and Nf with a shift of the formula to the left (i.e. P/i, S/i, etc.), ESR; The increase in neutrophils occurs at the compensatory stage, as soon as the depot is depleted, Nf ↓ (neutropenia).
- evaluate acid-base balance parameters: the amount of bicarbonate, buffer bases, O₂ and oxygen capacity of the blood, etc.
- OAM: proteinuria, hematuria, bacteriuria - all this will only indicate the degree of compensatory reaction and contamination.
- X-ray diagnostics: ↓mediastinal lymph nodes, focal/lobular/pseudolabular pneumonia, RDS (respiratory distress syndrome).
- Lumbar puncture for meningeal symptoms (stiff neck, positive Kering and Brudzinski symptoms), which reveals: 3-digit neutrophilic pleocytosis + [protein] + ↓[glu].
- Examination of bubo punctate / ulcers / carbuncle / sputum / nasopharyngeal smear / blood / urine / feces / cerebrospinal fluid - that is, where the symptoms dominate, and the biological material is sent for bacteriological and bacteriscopic examination - the preliminary result is in an hour, and the final after 12 hours (when plague stalactites appear, this makes the diagnosis indisputable).
- RPHA (passive hemagglutination reaction), RIF, ELISA, RNGA

If plague is suspected, laboratory tests are carried out in anti-plague suits, in specialized laboratory conditions, using specially designated dishes and containers, as well as with the mandatory availability of disinfectants.
Treatment of plague
Treatment is combined with bed rest and gentle nutrition (table A).
1. Etiotropic treatment (directed against the pathogen) - this stage should be started only with one suspicion of plague, without waiting for bacteriological confirmation. For a certain form, different combinations of drugs are used, alternating them with each other, the most successful combinations in this case:
- Ciftriaxone or Ciprofloxacin + streptomycin, or gentamicin, or rifampicin
- Rifampicin + Streptomycin
2. Pathogenetic treatment: combating acidosis, cardiovascular and respiratory failure, ITS and DIC syndrome. During this treatment, colloid solutions (reopolyglucin, plasma) and crystalloid solutions (10% glucose) are administered.
3. Symptomatic therapy as certain dominant symptoms appear.
Complications of the plague
Development of irreversible stages of ITS and DIC, decompensation of organs and systems, secondary bacterial complications, death.
Prevention of plague
Nonspecific: epidemiological surveillance of natural foci; reducing the number of rodents with disinsection; constant monitoring of the population at risk; preparing medical institutions and medical personnel to work with plague patients; prevention of import from other countries.
Specific: annual immunization with a live anti-plague vaccine of persons living in risk areas or traveling there; People who come into contact with plague patients, their belongings, or animal corpses are given emergency antibiotic prophylaxis with the same drugs used for treatment.
Post-infectious immunity is believed to be strong and lifelong, but cases of reinfection have been reported.
*National Infectious Disease Guidelines classify plague as a zoonotic disease, meaning one that cannot spread from person to person. But can this be considered legitimate, remembering the epidemic history of Europe in the 14th century, when in 1346-1351, out of a population of 100 million, only 70 million remained? I don’t think this characterization is appropriate, since only those diseases that are transmitted from animals are called “zoonosis.” to animals and humans is an “infectious dead end”, i.e. without the possibility of infecting other people, and “zooanthraponosis” implies infection not only between animals, but also between people.
General practitioner Shabanova I.E.
They also belong to the Ancient World. Thus, Rufus from Ephesus, who lived during the time of Emperor Trajan, referring to more ancient doctors (whose names have not reached us), described several cases of definitely bubonic plague in Libya, Syria and Egypt.
The Philistines did not calm down and for the third time transported the trophy of war, and with it the plague, to the city of Ascalon. All the Philistine rulers later gathered there - the kings of the five cities of Philistia - and they decided to return the ark to the Israelites, because they realized that this was the only way to prevent the spread of the disease. And chapter 5 ends with a description of the atmosphere that reigned in the doomed city. “And those who did not die were smitten with growths, so that the cry of the city went up to heaven” (1 Sam.). Chapter 6 depicts the council of all the rulers of the Philistines, to which priests and soothsayers were called. They advised to bring a trespass offering to God - to put gifts in the ark before returning it to the Israelites. “According to the number of the rulers of the Philistines, there are five golden growths and five golden mice that devastate the land; for the execution is one for all of you and for those who rule you” (1 Sam.). This biblical legend is interesting in many respects: it contains a hidden message about an epidemic that most likely swept through all five cities of Philistia. We could be talking about the bubonic plague, which affected people young and old and was accompanied by the appearance of painful growths in the groin - buboes. The most remarkable thing is that the Philistine priests apparently associated this disease with the presence of rodents: hence the golden statues of mice “ravaging the earth.”
There is another passage in the Bible that is considered to be a record of another instance of the plague. The Fourth Book of Kings (2 Kings) tells the story of the campaign of the Assyrian king Sennacherib, who decided to devastate Jerusalem. A huge army surrounded the city, but did not take control of it. And soon Sennacherib withdrew without a fight with the remnants of the army, in which the “Angel of the Lord” struck 185 thousand soldiers overnight (2 Kings).
Plague epidemics in historical times
Plague as a biological weapon
The use of the plague agent as a biological weapon has deep historical roots. In particular, events in ancient China and medieval Europe showed the use of the corpses of infected animals (horses and cows), human bodies by the Huns, Turks and Mongols to contaminate water sources and water supply systems. There are historical reports of cases of ejection of infected material during the siege of some cities (Siege of Kaffa).
Current state
Every year the number of people infected with the plague is about 2.5 thousand people, with no downward trend.
According to available data, according to the World Health Organization, from 1989 to 2004, about forty thousand cases were recorded in 24 countries, with a mortality rate of about 7% of the number of cases. In a number of countries in Asia (Kazakhstan, China, Mongolia and Vietnam), Africa (Congo, Tanzania and Madagascar), and the Western Hemisphere (USA, Peru), cases of human infection are recorded almost every year.
At the same time, on the territory of Russia, over 20 thousand people are at risk of infection every year in the territory of natural foci (with a total area of more than 253 thousand km²). For Russia, the situation is complicated by the annual identification of new cases in states neighboring Russia (Kazakhstan, Mongolia, China), and the importation of a specific carrier of the plague, fleas, through transport and trade flows from the countries of Southeast Asia. Xenopsylla cheopis .
From 2001 to 2006, 752 strains of the plague pathogen were recorded in Russia. At the moment, the most active natural foci are located in the territories of the Astrakhan region, the Kabardino-Balkarian and Karachay-Cherkess republics, the republics of Altai, Dagestan, Kalmykia, and Tyva. Of particular concern is the lack of systematic monitoring of the activity of outbreaks located in the Ingush and Chechen Republics.
In July 2016, in Russia, a ten-year-old boy with bubonic plague was taken to the hospital in the Kosh-Agach district of the Altai Republic.
In 2001-2003, 7 cases of plague were registered in the Republic of Kazakhstan (with one death), in Mongolia - 23 (3 deaths), in China in 2001-2002, 109 people fell ill (9 deaths). The forecast for the epizootic and epidemic situation in the natural foci of the Republic of Kazakhstan, China and Mongolia adjacent to the Russian Federation remains unfavorable.
At the end of August 2014, an outbreak of plague occurred again in Madagascar, which by the end of November 2014 had claimed 40 lives out of 119 cases.
Forecast
Under modern therapy, mortality in the bubonic form does not exceed 5-10%, but in other forms the recovery rate is quite high if treatment is started early. In some cases, a transient septic form of the disease is possible, which is poorly amenable to intravital diagnosis and treatment (“fulminant form of plague”).
Infection
The causative agent of plague is resistant to low temperatures, preserves well in sputum, but at a temperature of 55 ° C it dies within 10-15 minutes, and when boiled - almost instantly. The gate of infection is damaged skin (with a flea bite, as a rule, Xenopsylla cheopis), mucous membranes of the respiratory tract, digestive tract, conjunctiva.
Based on the main carrier, natural plague foci are divided into ground squirrels, marmots, gerbils, voles and pikas. In addition to wild rodents, the epizootic process sometimes includes so-called synanthropic rodents (in particular, rats and mice), as well as some wild animals (hares, foxes) that are the object of hunting. Among domestic animals, camels suffer from the plague.
In a natural outbreak, infection usually occurs through the bite of a flea that previously fed on a sick rodent. The likelihood of infection increases significantly when synanthropic rodents are included in the epizootic. Infection also occurs during hunting of rodents and their further processing. Massive diseases of people occur when a sick camel is slaughtered, skinned, butchered, or processed. An infected person, in turn, is a potential source of plague, from which the pathogen can be transmitted to another person or animal, depending on the form of the disease, by airborne droplets, contact or transmission.
Fleas are a specific carrier of the plague pathogen. This is due to the peculiarities of the digestive system of fleas: just before the stomach, the flea's esophagus forms a thickening - a goiter. When an infected animal (rat) is bitten, the plague bacterium settles in the flea’s crop and begins to multiply intensively, completely clogging it (the so-called “plague block”). Blood cannot enter the stomach, so the flea regurgitates the blood along with the pathogen back into the wound. And since such a flea is constantly tormented by a feeling of hunger, it moves from owner to owner in the hope of getting its share of blood and manages to infect a large number of people before dying (such fleas live no more than ten days, but experiments on rodents have shown that one flea can infect up to 11 hosts).
When a person is bitten by fleas infected with plague bacteria, a papule or pustule filled with hemorrhagic contents (cutaneous form) may appear at the site of the bite. The process then spreads through the lymphatic vessels without the appearance of lymphangitis. The proliferation of bacteria in the macrophages of the lymph nodes leads to their sharp increase, fusion and formation of a conglomerate (“bubo”). Further generalization of the infection, which is not strictly necessary, especially in the conditions of modern antibacterial therapy, can lead to the development of a septic form, accompanied by damage to almost all internal organs. From an epidemiological point of view, it is important that plague bacteremia develops, as a result of which a sick person himself becomes a source of infection through contact or transmission. However, the most important role is played by the “screening out” of infection into the lung tissue with the development of the pulmonary form of the disease. From the moment plague pneumonia develops, the pulmonary form of the disease is already transmitted from person to person - extremely dangerous, with a very rapid course.
Symptoms
The bubonic form of plague is characterized by the appearance of sharply painful conglomerates, most often in the inguinal lymph nodes on one side. The incubation period is 2-6 days (less often 1-12 days). Over the course of several days, the size of the conglomerate increases, and the skin over it may become hyperemic. At the same time, an increase in other groups of lymph nodes appears - secondary buboes. The lymph nodes of the primary focus undergo softening; upon puncture, purulent or hemorrhagic contents are obtained, microscopic analysis of which reveals a large number of gram-negative rods with bipolar staining. In the absence of antibacterial therapy, festering lymph nodes are opened. Then gradual healing of the fistula occurs. The severity of the patients' condition gradually increases by the 4-5th day, the temperature may be elevated, sometimes a high fever immediately appears, but at first the condition of the patients often remains generally satisfactory. This explains the fact that a person sick with bubonic plague can fly from one part of the world to another, considering himself healthy.
However, at any time, the bubonic form of plague can cause generalization of the process and turn into a secondary septic or secondary pulmonary form. In these cases, the condition of the patients very quickly becomes extremely serious. Symptoms of intoxication increase by the hour. The temperature after severe chills rises to high febrile levels. All signs of sepsis are noted: muscle pain, severe weakness, headache, dizziness, congestion of consciousness, up to its loss, sometimes agitation (the patient rushes about in bed), insomnia. With the development of pneumonia, cyanosis increases, a cough appears with the release of foamy, bloody sputum containing a huge amount of plague bacilli. It is this sputum that becomes the source of infection from person to person with the development of the now primary pneumonic plague.
Septic and pneumonic forms of plague occur, like any severe sepsis, with manifestations of disseminated intravascular coagulation syndrome: minor hemorrhages on the skin are possible, bleeding from the gastrointestinal tract is possible (vomiting of bloody masses, melena), severe tachycardia, rapid and requiring correction ( dopamine) drop in blood pressure. Auscultation reveals a picture of bilateral focal pneumonia.
Clinical picture
The clinical picture of the primary septic or primary pulmonary form is not fundamentally different from the secondary forms, but the primary forms often have a shorter incubation period - up to several hours.
Diagnosis
The most important role in diagnosis in modern conditions is played by epidemiological anamnesis. Arrival from zones endemic for plague (Vietnam, Burma, Bolivia, Ecuador, Karakalpakstan, etc.), or from anti-plague stations of a patient with the signs of the bubonic form described above or with signs of the most severe - with hemorrhages and bloody sputum - pneumonia with severe lymphadenopathy is for doctor of first contact is a sufficiently serious argument for taking all measures to localize the suspected plague and accurately diagnose it. It should be especially emphasized that in the conditions of modern drug prevention, the likelihood of illness among personnel who have been in contact with a coughing plague patient for some time is very small. Currently, there are no cases of primary pneumonic plague (that is, cases of infection from person to person) among medical personnel. An accurate diagnosis must be made using bacteriological studies. The material for them is the punctate of a suppurating lymph node, sputum, the patient’s blood, discharge from fistulas and ulcers.
Laboratory diagnosis is carried out using a fluorescent specific antiserum, which is used to stain smears of discharge from ulcers, punctate lymph nodes, and cultures obtained on blood agar.
Treatment
In the Middle Ages, the plague was practically not treated; actions were reduced mainly to cutting out or cauterizing the plague buboes. No one knew the real cause of the disease, so there was no idea how to treat it. Doctors tried to use the most bizarre means. One such drug included a mixture of 10-year-old molasses, finely chopped snakes, wine and 60 other ingredients. According to another method, the patient had to take turns sleeping on his left side, then on his right. Since the 13th century, attempts have been made to limit the plague epidemic through quarantines.
A turning point in plague treatment was reached in 1947, when Soviet doctors were the first in the world to use streptomycin to treat plague in Manchuria. As a result, all patients who were treated with streptomycin recovered, including a patient with pneumonic plague, who was already considered hopeless.
Treatment of plague patients is currently carried out using antibiotics, sulfonamides and medicinal anti-plague serum. Prevention of possible outbreaks of the disease consists of carrying out special quarantine measures in port cities, deratization of all ships that sail on international flights, creating special anti-plague institutions in steppe areas where rodents are found, identifying plague epizootics among rodents and combating them.
Anti-plague sanitary measures in Russia
If plague is suspected, the sanitary-epidemiological station of the area is immediately notified. The notification is filled out by the doctor who suspects an infection, and its forwarding is ensured by the chief physician of the institution where such a patient was found.
The patient should be immediately hospitalized in the infectious diseases hospital. A doctor or paramedical worker of a medical institution, upon discovering a patient or suspected of having the plague, is obliged to stop further admission of patients and prohibit entry and exit from the medical institution. While remaining in the office or ward, the medical worker must inform the chief physician in a way accessible to him about the identification of the patient and demand anti-plague suits and disinfectants.
In cases of receiving a patient with lung damage, before putting on a full anti-plague suit, the medical worker is obliged to treat the mucous membranes of the eyes, mouth and nose with streptomycin solution. If there is no cough, you can limit yourself to treating your hands with a disinfectant solution. After taking measures to separate the sick person from the healthy, a list of people who had contact with the patient is compiled in a medical institution or at home, indicating their last name, first name, patronymic, age, place of work, profession, home address.
Until the consultant from the anti-plague institution arrives, the health worker remains in the outbreak. The issue of its isolation is decided in each specific case individually. The consultant takes the material for bacteriological examination, after which specific treatment of the patient with antibiotics can begin.
When identifying a patient on a train, plane, ship, airport, or railway station, the actions of medical workers remain the same, although the organizational measures will be different. It is important to emphasize that isolation of a suspicious patient from others should begin immediately after identification.
The chief doctor of the institution, having received a message about the identification of a patient suspected of plague, takes measures to stop communication between the hospital departments and the floors of the clinic, and prohibits leaving the building where the patient was found. At the same time, organizes the transmission of emergency messages to a higher organization and the anti-plague institution. The form of information can be arbitrary with the obligatory presentation of the following data: last name, first name, patronymic, age of the patient, place of residence, profession and place of work, date of detection, time of onset of the disease, objective data, preliminary diagnosis, primary measures taken to localize the outbreak, position and the name of the doctor who diagnosed the patient. Along with the information, the manager requests consultants and the necessary assistance.
However, in some situations, it may be more appropriate to carry out hospitalization (before establishing an accurate diagnosis) in the institution where the patient is at the time of the suspicion that he has plague. Therapeutic measures are inseparable from the prevention of infection of personnel, who must immediately put on 3-layer gauze masks, shoe covers, a scarf made of 2 layers of gauze that completely covers the hair, and protective glasses to prevent splashes of sputum from entering the mucous membrane of the eyes. According to the rules established in the Russian Federation, personnel must wear an anti-plague suit or use special means of anti-infective protection with similar properties. All personnel who had contact with the patient remain to provide further assistance to him. A special medical post isolates the compartment where the patient and the personnel treating him are located from contact with other people. The isolated compartment should include a toilet and a treatment room. All personnel immediately receive prophylactic antibiotic treatment, continuing throughout the days they spend in isolation.
Treatment of plague is complex and includes the use of etiotropic, pathogenetic and symptomatic agents. For the treatment of plague, the most effective antibiotics are the streptomycin series: streptomycin, dihydrostreptomycin, pasomycin. In this case, streptomycin is most widely used. For the bubonic form of plague, the patient is administered streptomycin intramuscularly 3-4 times a day (daily dose of 3 g), tetracycline antibiotics (vibromycin, morphocycline) intramuscularly at 4 g/day. In case of intoxication, saline solutions and hemodez are administered intravenously. A drop in blood pressure in the bubonic form should in itself be regarded as a sign of generalization of the process, a sign of sepsis; in this case, there is a need to carry out resuscitation measures, administer dopamine, and install a permanent catheter. For pneumonic and septic forms of plague, the dose of streptomycin is increased to 4-5 g/day, and tetracycline - to 6 g. For forms resistant to streptomycin, chloramphenicol succinate can be administered up to 6-8 g intravenously. When the condition improves, the dose of antibiotics is reduced: streptomycin - up to 2 g/day until the temperature normalizes, but for at least 3 days, tetracyclines - up to 2 g/day daily orally, chloramphenicol - up to 3 g/day, for a total of 20-25 g. Biseptol is also used with great success in the treatment of plague.
In case of pulmonary, septic form, development of hemorrhage, they immediately begin to relieve the syndrome of disseminated intravascular coagulation: plasmapheresis is performed (intermittent plasmapheresis in plastic bags can be carried out on any centrifuge with special or air cooling with a capacity of its glasses of 0.5 liters or more) in the volume removed plasma 1-1.5 liters when replaced with the same amount of fresh frozen plasma. In the presence of hemorrhagic syndrome, daily administration of fresh frozen plasma should not be less than 2 liters. Until the acute manifestations of sepsis are relieved, plasmapheresis is performed daily. The disappearance of signs of hemorrhagic syndrome and stabilization of blood pressure, usually in sepsis, are grounds for stopping plasmapheresis sessions. At the same time, the effect of plasmapheresis in the acute period of the disease is observed almost immediately, signs of intoxication decrease, the need for dopamine to stabilize blood pressure decreases, muscle pain subsides, and shortness of breath decreases.
The team of medical personnel providing treatment to a patient with pneumonic or septic form of plague must include an intensive care specialist.
See also
- Inquisitio
- Plague (group)
Notes
- Disease Ontology release 2019-05-13 - 2019-05-13 - 2019.
- Jared Diamond, Guns, Germs and Steel. The Fates of Human Societies.
- , With. 142.
- Plague
- , With. 131.
- Plague - for doctors, students, patients, medical portal, abstracts, cheat sheets for doctors, disease treatment, diagnosis, prevention
- , With. 7.
- , With. 106.
- , With. 5.
- Papagrigorakis, Manolis J.; Yapijakis, Christos; Synodinos, Philippos N.; Baziotopoulou-Valavani, Effie (2006). “DNA examination of ancient dental pulp incriminates typhoid fever as a probable cause of the Plague of Athens” . International Journal of Infectious Diseases. 10 (3): 206-214.
Plague
What is Plague -
Plague- an acute, especially dangerous zoonotic transmissible infection with severe intoxication and serous-hemorrhagic inflammation in the lymph nodes, lungs and other organs, as well as the possible development of sepsis.
Brief historical information
There is no other infectious disease in the history of mankind that would lead to such colossal devastation and mortality among the population as the plague. Since ancient times, information has been preserved about the plague, which occurred in people in the form of epidemics with a large number of deaths. It was noted that plague epidemics developed as a result of contact with sick animals. At times, the spread of the disease was pandemic-like. There are three known plague pandemics. The first, known as the Plague of Justinian, raged in Egypt and the Eastern Roman Empire from 527-565. The second, called the “great” or “black” death, in 1345-1350. covered Crimea, the Mediterranean and Western Europe; this most devastating pandemic has claimed about 60 million lives. The third pandemic began in 1895 in Hong Kong and then spread to India, where over 12 million people died. At its very beginning, important discoveries were made (the pathogen was isolated, the role of rats in the epidemiology of the plague was proven), which made it possible to organize prevention on a scientific basis. The causative agent of the plague was discovered by G.N. Minkh (1878) and independently of him A. Yersin and S. Kitazato (1894). Since the 14th century, the plague has repeatedly visited Russia in the form of epidemics. Working on outbreaks to prevent the spread of the disease and treat patients, Russian scientists D.K. made a great contribution to the study of the plague. Zabolotny, N.N. Klodnitsky, I.I. Mechnikov, N.F. Gamaleya and others. In the 20th century N.N. Zhukov-Verezhnikov, E.I. Korobkova and G.P. Rudnev developed the principles of pathogenesis, diagnosis and treatment of plague patients, and also created an anti-plague vaccine.
What provokes / Causes of the Plague:
The causative agent is a gram-negative, non-motile, facultative anaerobic bacterium Y. pestis of the Yersinia genus of the Enterobacteriaceae family. In many morphological and biochemical characteristics, the plague bacillus is similar to the pathogens of pseudotuberculosis, yersiniosis, tularemia and pasteurellosis, which cause severe diseases in both rodents and humans. It is distinguished by pronounced polymorphism, the most typical are ovoid rods that stain bipolarly. There are several subspecies of the pathogen, differing in virulence. Grows on regular nutrient media with the addition of hemolyzed blood or sodium sulfite to stimulate growth. Contains more than 30 antigens, exo- and endotoxins. Capsules protect bacteria from absorption by polymorphonuclear leukocytes, and V- and W-antigens protect them from lysis in the cytoplasm of phagocytes, which ensures their intracellular reproduction. The causative agent of plague is well preserved in the excreta of patients and objects of the external environment (in the pus of a bubo it persists for 20-30 days, in the corpses of people, camels, rodents - up to 60 days), but is highly sensitive to sunlight, atmospheric oxygen, elevated temperature, environmental reactions (especially acidic), chemicals (including disinfectants). Under the influence of mercuric chloride at a dilution of 1:1000, it dies in 1-2 minutes. Tolerates low temperatures and freezing well.
A sick person can, under certain conditions, become a source of infection: with the development of pneumonic plague, direct contact with the purulent contents of a plague bubo, as well as as a result of flea infection on a patient with plague septicemia. The corpses of people who died from the plague are often the direct cause of infection of others. Patients with pneumonic plague are especially dangerous.
Transmission mechanism diverse, most often transmissible, but airborne droplets are also possible (with pneumonic forms of plague, infection in laboratory conditions). The carriers of the pathogen are fleas (about 100 species) and some types of ticks, which support the epizootic process in nature and transmit the pathogen to synanthropic rodents, camels, cats and dogs, which can carry infected fleas to human habitation. A person becomes infected not so much through a flea bite as after rubbing its feces or masses regurgitated during feeding into the skin. Bacteria that multiply in the intestines of a flea secrete coagulase, which forms a “plug” (plague block) that prevents the flow of blood into its body. Attempts by a hungry insect to suck blood are accompanied by regurgitation of infected masses onto the surface of the skin at the site of the bite. These fleas are hungry and often try to suck the animal's blood. The contagiousness of fleas lasts on average about 7 weeks, and according to some data - up to 1 year.
Contact (through damaged skin and mucous membranes) when cutting carcasses and processing the skins of killed infected animals (hares, foxes, saigas, camels, etc.) and nutritional (by eating their meat) routes of infection with plague are possible.
The natural susceptibility of people is very high, absolute in all age groups and through any route of infection. After an illness, relative immunity develops, which does not protect against re-infection. Repeated cases of the disease are not uncommon and are no less severe than the primary ones.
Basic epidemiological signs. Natural foci of plague occupy 6-7% of the globe's land mass and are registered on all continents, excluding Australia and Antarctica. Every year, several hundred cases of plague in humans are recorded worldwide. In the CIS countries, 43 natural plague foci have been identified with a total area of more than 216 million hectares, located in lowland (steppe, semi-desert, desert) and high-mountain regions. There are two types of natural foci: foci of “wild” and foci of rat plague. In natural foci, plague manifests itself as an epizootic among rodents and lagomorphs. Infection from rodents that do not sleep in winter (marmots, gophers, etc.) occurs in the warm season, while from rodents and lagomorphs that do not sleep in winter (gerbils, voles, pikas, etc.), infection has two seasonal peaks, which is associated with breeding periods animals. Men get sick more often than women due to professional activities and stay in a natural plague focus (transhumance, hunting). In anthropurgic foci, the role of infection reservoir is performed by black and gray rats. The epidemiology of bubonic and pneumonic plague has significant differences in its most important features. Bubonic plague is characterized by a relatively slow increase in disease, while pneumonic plague, due to the easy transmission of bacteria, can become widespread in a short time. Patients with the bubonic form of plague are low-contagious and practically non-infectious, since their secretions do not contain pathogens, and there are few or no pathogens in the material from the opened buboes. When the disease passes into the septic form, as well as when the bubonic form is complicated by secondary pneumonia, when the pathogen can be transmitted by airborne droplets, severe epidemics of primary pneumonic plague develop with very high contagiousness. Typically, pneumonic plague follows bubonic plague, spreads along with it and quickly becomes the leading epidemiological and clinical form. Recently, the idea that the plague causative agent can remain in the soil for a long time in an uncultivated state has been intensively developed. Primary infection of rodents can occur when digging holes in infected areas of soil. This hypothesis is based both on experimental studies and observations on the futility of searching for the pathogen among rodents and their fleas during inter-epizootic periods.
Pathogenesis (what happens?) during the Plague:
Human adaptation mechanisms are practically not adapted to resist the introduction and development of the plague bacillus in the body. This is explained by the fact that the plague bacillus multiplies very quickly; bacteria produce large quantities of permeability factors (neuraminidase, fibrinolysin, pesticin), antiphagins that suppress phagocytosis (F1, HMWPs, V/W-Ar, PH6-Ag), which contributes to rapid and massive lymphogenous and hematogenous dissemination primarily into mononuclear organs phagocytic system with its subsequent activation. Massive antigenemia, the release of inflammatory mediators, including shockogenic cytokines, leads to the development of microcirculatory disorders, DIC syndrome, followed by infectious-toxic shock.
The clinical picture of the disease is largely determined by the site of introduction of the pathogen, penetrating through the skin, lungs or gastrointestinal tract.
The pathogenesis of plague includes three stages. First, the pathogen disseminates lymphogenously from the site of introduction to the lymph nodes, where it lingers for a short time. In this case, a plague bubo is formed with the development of inflammatory, hemorrhagic and necrotic changes in the lymph nodes. The bacteria then quickly enter the bloodstream. At the stage of bacteremia, severe toxicosis develops with changes in the rheological properties of the blood, microcirculation disorders and hemorrhagic manifestations in various organs. And finally, after the pathogen overcomes the reticulohistiocytic barrier, it disseminates to various organs and systems with the development of sepsis.
Microcirculatory disorders cause changes in the heart muscle and blood vessels, as well as in the adrenal glands, which causes acute cardiovascular failure.
With the aerogenic route of infection, the alveoli are affected, and an inflammatory process with elements of necrosis develops in them. Subsequent bacteremia is accompanied by intense toxicosis and the development of septic-hemorrhagic manifestations in various organs and tissues.
The antibody response to plague is weak and forms in the late stages of the disease.
Symptoms of the Plague:
The incubation period is 3-6 days (in epidemics or septic forms it is reduced to 1-2 days); The maximum incubation period is 9 days.
Characterized by an acute onset of the disease, expressed by a rapid increase in body temperature to high numbers with stunning chills and the development of severe intoxication. Patients typically complain of pain in the sacrum, muscles and joints, and headaches. Vomiting (often bloody) and excruciating thirst occur. Already from the first hours of the disease, psychomotor agitation develops. Patients are restless, overly active, try to run (“runs like crazy”), they experience hallucinations and delusions. Speech becomes slurred and gait is unsteady. In more rare cases, lethargy, apathy are possible, and weakness reaches such a degree that the patient cannot get out of bed. Externally, hyperemia and puffiness of the face and scleral injection are noted. There is an expression of suffering or horror on the face (“plague mask”). In more severe cases, a hemorrhagic rash may appear on the skin. Very characteristic signs of the disease are thickening and coating of the tongue with a thick white coating (“chalky tongue”). From the cardiovascular system, pronounced tachycardia (up to embryocardia), arrhythmia and a progressive drop in blood pressure are noted. Even with local forms of the disease, tachypnea, as well as oliguria or anuria, develop.
This symptomatology manifests itself, especially in the initial period, in all forms of plague.
According to the clinical classification of plague proposed by G.P. Rudnev (1970), distinguish local forms of the disease (cutaneous, bubonic, cutaneous-bubonic), generalized forms (primary septic and secondary septic), externally disseminated forms (primary pulmonary, secondary pulmonary and intestinal).
Skin form. The formation of a carbuncle at the site of introduction of the pathogen is characteristic. Initially, a sharply painful pustule with dark red contents appears on the skin; it is localized on the edematous subcutaneous tissue and is surrounded by a zone of infiltration and hyperemia. After opening the pustule, an ulcer with a yellowish bottom is formed, which tends to increase in size. Subsequently, the bottom of the ulcer is covered with a black scab, after which scarring is formed.
Bubonic form. The most common form of plague. Characterized by damage to lymph nodes regional to the site of introduction of the pathogen - inguinal, less often axillary and very rarely cervical. Usually the buboes are single, less often multiple. Against the background of severe intoxication, pain occurs in the area of the future localization of the bubo. After 1-2 days, you can palpate sharply painful lymph nodes, first of a hard consistency, and then softening and becoming doughy. The nodes merge into a single conglomerate, inactive due to the presence of periadenitis, fluctuating upon palpation. The duration of the height of the disease is about a week, after which a period of convalescence begins. Lymph nodes can resolve on their own or become ulcerated and sclerotic due to serous-hemorrhagic inflammation and necrosis.
Cutaneous bubonic form. It is a combination of skin lesions and changes in the lymph nodes.
These local forms of the disease can develop into secondary plague sepsis and secondary pneumonia. Their clinical characteristics do not differ from primary septic and primary pulmonary forms of plague, respectively.
Primary septic form. It occurs after a short incubation period of 1-2 days and is characterized by lightning-fast development of intoxication, hemorrhagic manifestations (hemorrhages in the skin and mucous membranes, gastrointestinal and renal bleeding), and the rapid formation of a clinical picture of infectious-toxic shock. Without treatment, it is fatal in 100% of cases.
Primary pulmonary form. Develops during aerogenic infection. The incubation period is short, from several hours to 2 days. The disease begins acutely with manifestations of the intoxication syndrome characteristic of the plague. On the 2-3rd day of illness, a severe cough appears, sharp pain in the chest, and shortness of breath occur. The cough is accompanied by the release of first glassy and then liquid, foamy, bloody sputum. Physical data from the lungs are scant; X-rays show signs of focal or lobar pneumonia. Cardiovascular failure increases, expressed in tachycardia and a progressive drop in blood pressure, and the development of cyanosis. In the terminal stage, patients first develop a stuporous state, accompanied by increased shortness of breath and hemorrhagic manifestations in the form of petechiae or extensive hemorrhages, and then coma.
Intestinal form. Against the background of intoxication syndrome, patients experience severe abdominal pain, repeated vomiting and diarrhea with tenesmus and copious mucous-bloody stools. Since intestinal manifestations can be observed in other forms of the disease, until recently the question of the existence of intestinal plague as an independent form, apparently associated with enteral infection, remains controversial.
Differential diagnosis
Cutaneous, bubonic and cutaneous bubonic forms of plague should be distinguished from tularemia, carbuncles, various lymphadenopathy, pulmonary and septic forms - from inflammatory lung diseases and sepsis, including meningococcal etiology.
With all forms of plague, already in the initial period, rapidly increasing signs of severe intoxication are alarming: high body temperature, tremendous chills, vomiting, excruciating thirst, psychomotor agitation, restlessness, delirium and hallucinations. When examining patients, attention is drawn to slurred speech, an unsteady gait, a puffy, hyperemic face with scleral injection, an expression of suffering or horror (“plague mask”), and a “chalky tongue.” Signs of cardiovascular failure, tachypnea rapidly increase, and oliguria progresses.
Cutaneous, bubonic and cutaneous bubonic forms of plague are characterized by severe pain at the site of the lesion, stages in the development of the carbuncle (pustule - ulcer - black scab - scar), pronounced phenomena of periadenitis during the formation of the plague bubo.
Pulmonary and septic forms are distinguished by the lightning-fast development of severe intoxication, pronounced manifestations of hemorrhagic syndrome, and infectious-toxic shock. If the lungs are affected, sharp pain in the chest and severe cough, separation of glassy and then liquid foamy bloody sputum are noted. The scanty physical data do not correspond to the general extremely serious condition.
Diagnosis of Plague:
Laboratory diagnostics
Based on the use of microbiological, immunoserological, biological and genetic methods. The hemogram shows leukocytosis, neutrophilia with a shift to the left, and an increase in ESR. Isolation of the pathogen is carried out in specialized high-security laboratories for working with pathogens of particularly dangerous infections. Studies are carried out to confirm clinically significant cases of the disease, as well as to examine people with elevated body temperature who are at the source of infection. Material from the sick and dead is subjected to bacteriological examination: punctates from buboes and carbuncles, discharge from ulcers, sputum and mucus from the oropharynx, blood. The passage is carried out on laboratory animals (guinea pigs, white mice), which die on the 5-7th day after infection.
Among the serological methods used are RNGA, RNAT, RNAG and RTPGA, ELISA.
Positive PCR results 5-6 hours after its administration indicate the presence of specific DNA of the plague microbe and confirm the preliminary diagnosis. The final confirmation of the plague etiology of the disease is the isolation of a pure culture of the pathogen and its identification.
Plague treatment:
Plague patients are treated only in hospital settings. The choice of drugs for etiotropic therapy, their doses and regimens of use is determined by the form of the disease. The course of etiotropic therapy for all forms of the disease is 7-10 days. In this case the following is used:
for the skin form - cotrimoxazole 4 tablets per day;
for the bubonic form - chloramphenicol at a dose of 80 mg/kg/day and at the same time streptomycin at a dose of 50 mg/kg/day; drugs are administered intravenously; Tetracycline is also effective;
in pulmonary and septic forms of the disease, the combination of chloramphenicol with streptomycin is supplemented with the administration of doxycycline at a dose of 0.3 g/day or tetracycline at a dose of 4-6 g/day orally.
At the same time, massive detoxification therapy is carried out (fresh frozen plasma, albumin, rheopolyglucin, hemodez, intravenous crystalloid solutions, extracorporeal detoxification methods), drugs are prescribed to improve microcirculation and repair (trental in combination with solcoseryl, picamilon), forcing diuresis, as well as cardiac glycosides, vascular and respiratory analeptics, antipyretics and symptomatic agents.
The success of treatment depends on the timeliness of therapy. Etiotropic drugs are prescribed at the first suspicion of plague, based on clinical and epidemiological data.
Prevention of Plague:
Epidemiological surveillance
The volume, nature and direction of preventive measures are determined by the forecast of the epizootic and epidemic situation regarding plague in specific natural foci, taking into account data on tracking the movement of morbidity in all countries of the world. All countries are required to report to WHO about the emergence of plague diseases, the movement of morbidity, epizootics among rodents and measures to combat infection. The country has developed and operates a system for certification of natural plague foci, which made it possible to carry out epidemiological zoning of the territory.
Indications for preventive immunization of the population are an epizootic of plague among rodents, identification of domestic animals suffering from plague, and the possibility of infection being brought in by a sick person. Depending on the epidemic situation, vaccination is carried out in a strictly defined territory to the entire population (universally) and selectively to particularly endangered contingents - persons who have permanent or temporary connections with the territories where the epizootic is observed (livestock breeders, agronomists, hunters, harvesters, geologists, archaeologists, etc.). d.). In case of detection of a plague patient, all medical and preventive institutions must have a certain supply of medicines and means of personal protection and prevention, as well as a scheme for notifying personnel and transmitting information vertically. Measures to prevent people from becoming infected with plague in enzootic areas, people working with pathogens of particularly dangerous infections, as well as preventing the spread of infection beyond the foci to other areas of the country are carried out by anti-plague and other health care institutions.
Activities in the epidemic outbreak
When a person sick with plague or suspected of this infection appears, urgent measures are taken to localize and eliminate the outbreak. The boundaries of the territory where certain restrictive measures (quarantine) are introduced are determined based on the specific epidemiological and epizootological situation, possible operating factors of infection transmission, sanitary and hygienic conditions, intensity of population migration and transport connections with other territories. The general management of all activities in the plague outbreak is carried out by the Emergency Anti-Epidemic Commission. At the same time, the anti-epidemic regime is strictly observed using anti-plague suits. Quarantine is introduced by decision of the Emergency Anti-Epidemic Commission, covering the entire territory of the outbreak.
Patients with plague and patients suspected of having this disease are hospitalized in specially organized hospitals. Transportation of a plague patient must be carried out in accordance with current sanitary rules for biological safety. Patients with bubonic plague are placed in groups of several people in a room, while patients with the pulmonary form are placed only in separate rooms. Patients with bubonic plague are discharged no earlier than 4 weeks, with pneumonic plague - no earlier than 6 weeks from the date of clinical recovery and negative results of bacteriological examination. After the patient is discharged from the hospital, he is placed under medical supervision for 3 months.
Current and final disinfection is carried out in the outbreak. Persons who came into contact with plague patients, corpses, contaminated things, who participated in the forced slaughter of a sick animal, etc., are subject to isolation and medical observation (6 days). For pneumonic plague, individual isolation (for 6 days) and prophylaxis with antibiotics (streptomycin, rifampicin, etc.) are carried out for all persons who may have become infected.
Which doctors should you contact if you have Plague:
Is something bothering you? Do you want to know more detailed information about the Plague, its causes, symptoms, methods of treatment and prevention, the course of the disease and diet after it? Or do you need an inspection? You can make an appointment with a doctor– clinic Eurolab always at your service! The best doctors will examine you, study external signs and help you identify the disease by symptoms, advise you and provide the necessary assistance and make a diagnosis. You can also call a doctor at home. Clinic Eurolab open for you around the clock.
How to contact the clinic:
Phone number of our clinic in Kyiv: (+38 044) 206-20-00 (multi-channel). The clinic secretary will select a convenient day and time for you to visit the doctor. Our coordinates and directions are indicated. Look in more detail about all the clinic’s services on it.
(+38 044) 206-20-00
If you have previously performed any research, Be sure to take their results to a doctor for consultation. If the studies have not been performed, we will do everything necessary in our clinic or with our colleagues in other clinics.
At yours? It is necessary to take a very careful approach to your overall health. People don't pay enough attention symptoms of diseases and do not realize that these diseases can be life-threatening. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, it is too late to treat them. Each disease has its own specific signs, characteristic external manifestations - the so-called symptoms of the disease. Identifying symptoms is the first step in diagnosing diseases in general. To do this, you just need to do it several times a year. be examined by a doctor, in order not only to prevent a terrible disease, but also to maintain a healthy spirit in the body and the organism as a whole.
If you want to ask a doctor a question, use the online consultation section, perhaps you will find answers to your questions there and read self care tips. If you are interested in reviews about clinics and doctors, try to find the information you need in the section. Also register on the medical portal Eurolab to be constantly aware of the latest news and information updates on the site, which will be automatically sent to you by email.





