13 years 10 pet 5 pet 2 years 1 year b months Fig. 28. Terms of formation permanent teeth(scheme). the upper permanent teeth are as follows: Mj, I, 1 2, P 1 (P 2, C; M 2, M 3, lower permanent teeth: M s, I, 1 2, C, P, P 2> M 2, M 3 ,
It should be noted that in the process of eruption, permanent teeth first move under the roots of milk teeth and are located in connective tissue capsules, which is clearly seen on orthopanthograms in children 7-11 years old.
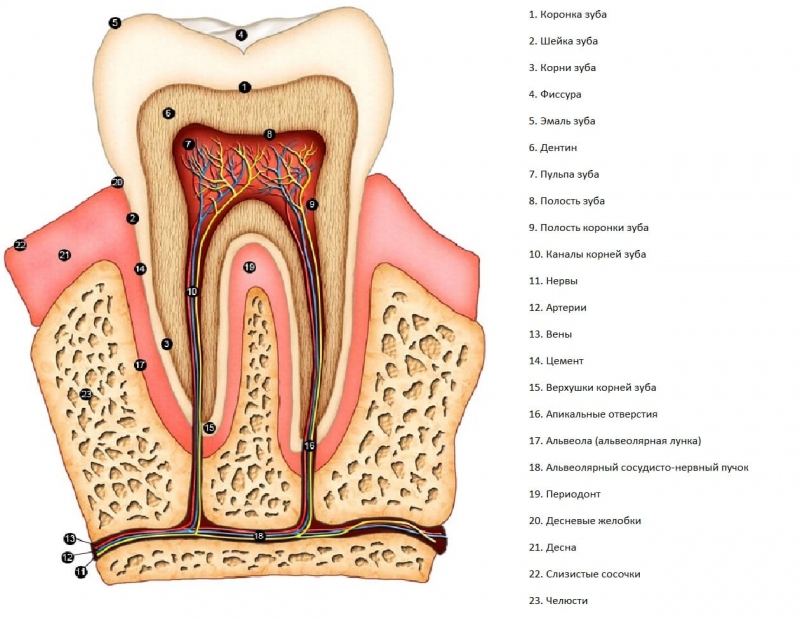
What are the different parts of a tooth? Crown - top part tooth and the only part that you can usually see. For example, anterior teeth are sharp and chisel for cutting, while molars have flat surfaces for grinding. Without correct cleaning and brushing teeth, tartar and tartar can build up on the gums, leading to gingivitis and gum disease. The root is about two-thirds of the tooth and holds the tooth in place. Enamel is the deepest layer of a tooth. Enamel is the hardest, most mineralized tissue in the body, but it can be damaged by decay if the teeth are not cared for properly. Dentin is the layer of the tooth under the enamel. If decay is able to move through the enamel, then it attacks the dentin, where millions of tiny tubes lead directly to the dental pulp. Pulp is the soft tissue found in the center of all teeth, where there are nerve tissue and blood vessels. reaches the pulp, you usually feel pain. The root is the part of the tooth that is embedded in the bone. ... What are the different types of teeth?
During this period, the roots of deciduous teeth undergo resorption and ultimately decay. Nutrition milk tooth broken, the crown falls out, opening the way for the permanent tooth.
In this case, milk incisors and canines are replaced by permanent teeth of the same name. In place of the milk molars, permanent premolars grow, and the permanent large molars erupt behind the milk teeth of the same name.
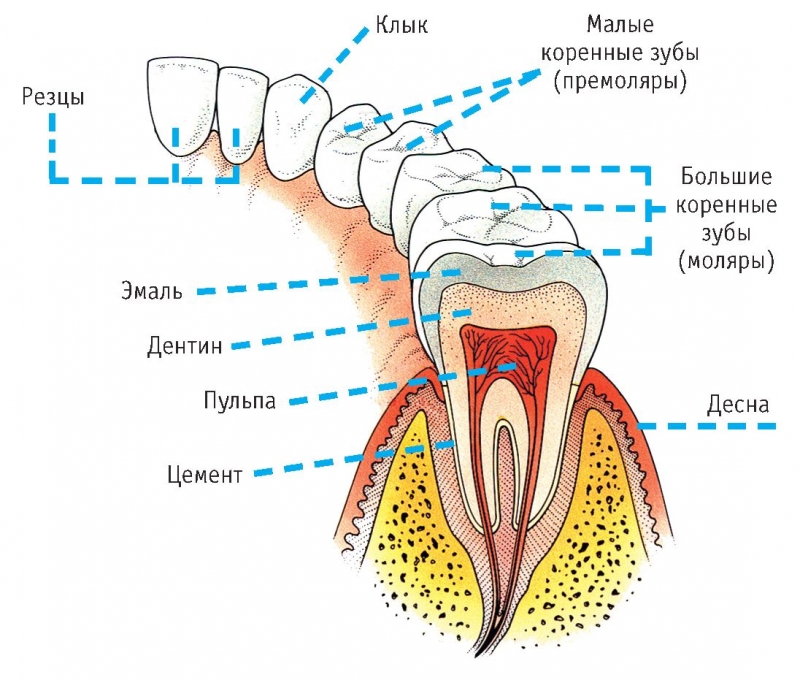
Each tooth has a specific job or function. Incisors - Sharp, chisel-shaped front teeth used for cutting food products... Canines - Sometimes called cusps, these teeth are point-shaped and are used to tear apart food. Premolars - These teeth have two pointed tips on their biting surface and are sometimes referred to as bicuspids. Molars - Used for grinding, these teeth have multiple cusps on the biting surface. 
Premolars are designed to crush and rupture. ... Although the mouth is a small part of our overall anatomy, it is filled with many parts and players, all of which work together to help you eat, drink, speak, and have a radiant smile.
It should be noted that the timing of the eruption of permanent teeth can vary significantly, which is determined individual characteristics(hereditary) or external influences (dietary habits, diseases). It is known that girls are ahead of boys in terms of teething rates. V last years in many countries, there is an earlier eruption of permanent teeth, which is explained by the phenomenon of acceleration.
The key players are incisors, canines, premolars, molars, crowns, gum line, root, enamel, dentin and cellulose. What are the different types of teeth. Here short review different types teeth in the middle mouth. Canines - Sometimes called cusps, these teeth are point-shaped and are used to tear and grab food. Molars - Used to grind and chew food, these teeth have multiple cusps on the biting surface to aid in this process. Premolars are designed to crush and break food. ... Each tooth has several separate parts; here is a quick overview of each part.
The average data on the number of permanent teeth in children of different ages are as follows: at 7 years old - in boys - 5 teeth; girls have 6 teeth; at 12 years old - boys have 18 teeth; girls have 21 teeth.
The development and eruption of permanent teeth contributes to an increase in the size of the jaws and face in the sagittal direction, due to which a facial profile is formed by the age of 15, i.e. the facial skeleton is stabilized.
Enamel is the outer and hardest part of the tooth and has the most mineralized tissue in the body. If decay penetrates the enamel, it attacks the dentin, where millions of tiny tubes lead directly to the dental pulp. Cellulose is a soft tissue found in the center of all teeth, where nerve tissue and blood vessels are located. If tooth decay reaches the pulp, you usually experience pain and may require a root canal procedure.
- It can be damaged by decay if the teeth are not properly cared for.
- Dentin is the layer of the tooth underneath the enamel.
2.4. Wear of teeth
During the functioning of the teeth, they gradually wear out, called tooth wear. The degree of wear can be different, which is associated with age, food, and also with the individual characteristics of people. The age of a person can be determined by the wear of the teeth.
The abrasion of permanent teeth is expressed in points: 0 - complete absence abrasion; 1 - the appearance of polished surfaces on the crowns, smoothness and roundness of the tops of the tubercles (16-18 years old); 2 - the appearance of areas of dentin on the cutting edges and tubercles (2030 years); 3 - the appearance of large areas of dentin with the erasure of all protruding parts of the crown; the enamel is preserved only in the depths of the grooves and pits (30-50 years); 4 - complete erasure of the enamel on the chewing surface, partial erasure of the crown (40-60 le g); 5 - erasing half of the crown (60-70 years old); 6 - complete erasure of the crown to the level of the neck (60 years and more).
They are not made of bone like everyone else, but they have their own unique structure that allows them to break down food. Tooth enamel is the most mineralized tissue in the body, composed primarily of the mountain mineral hydroxyapatite. Some animals have the ability to replace their teeth throughout their lives, as teeth can be lost due to injury or illness. Humans have two sets of teeth: baby teeth, which loosen and fall out until adulthood, and adult teeth, which remain in place in adulthood.
Temporary teeth also undergo abrasion, which is sharply expressed by the period of tooth change. 3. BLOOD SUPPLY AND INERVATION OF THE TEETH Blood supply to the teeth is carried out by the branches of the maxillary artery.
To the teeth upper jaw fit the anterior superior alveolar arteries, aa. alveolares superiores anteriores (from a. infraorbitalis) for the anterior and posterior superior alveolar arteries, aa. alveolares superiores posteriores (from a. maxillaris) for back molars.
The shape and number of an animal's teeth differs depending on what they are eating. Here, we will discuss the functions of different types of teeth, as well as the structure and different tissues that make up human teeth. Teeth help animals get food and break it down for efficient digestion. Animals that lose teeth are usually unable to swallow enough nutrients, to survive.
Upper and lower dentition. Strength in unity
The specific mechanical functions that teeth must perform depend on the food source of the animal. The animal may need to pierce the skin and rip meat, grind fibrous vegetables, or do some combination of the two. Predators often boast sharp, sharp, or even jagged teeth to help them shoot down prey and eat raw meat.
Smaller branches extend from the alveolar arteries: dental, rami dentales, to the teeth; gingival, rami gingivales, "to the gums and interalveolar, rami interalveolares, to the walls of the dental holes.
The lower alveolar artery branches off to the teeth of the lower jaw from the maxillary artery, a. alveolaris inferior, going in the mandibular canal, where it gives off the dental branches, rami dentales, to the teeth and interalveolar branches, rami interalveolares, to the gums and walls of the dental alveoli.
On the other hand, herbivores have long, sharp incisors in the front of their mouth to help cut plant-sized pieces, as well as molars with wide, textured surfaces at the back of their mouths that grind and break down plant matter to facilitate digestion.
People eat both meat and various plant substances. As a result, we have several types of teeth that are good for decay. different types food. Sharp, sharp "dog" teeth that can be used to tear pieces of meat and other foods. Molars and pre-molars, which suppress plant matter and other products in the pulp. Front teeth or incisors that cut food into bite-sized pieces. ... Structure human tooth includes the following fabrics.
Dental arteries enter root canals through the apical foramen and branch in the pulp of the tooth. Accompanying arteries and veins of the same name carry out the outflow of blood from the teeth into the pterygoid venous plexus.
The innervation of the teeth is carried out by sensitive fibers trigeminal nerve and sympathetic fibers extending from the upper cervical knot sympathetic trunk.
Enamel is a tough, calcified outer coating that is used to break down food. Enamel consists mainly of a matrix of hydroxyapatite, a mineral of crystalline calcium phosphate that is created by the cells of the body during the development of teeth. This tissue attaches the tooth to the periodontal ligaments that hold the tooth firmly in the jawbone. Cellulose, which contains blood vessels and nerves used to maintain dental health and prevent dangerous injuries and infections. Teeth are often destroyed by dentists in the following main regions.
The teeth of the upper jaw innervate the upper alveolar nerves, which branch off from the infraorbital nerve, n. Infraorbitalis (a branch of n. Maxillaris). The front teeth - incisors and canines - innervate the anterior branches, rami alveolares superiores anteriores, the middle branch, ramus alveolaris medius, goes to the premolars, the molars innervate the posterior branches, rami alveolares superiores posteriores.
All branches of the upper alveolar nerves form the upper dental plexus, plexus dentalis superior, from which the upper dental branches extend, rr. dentales superiores, K teeth, and upper gingival branches, rr. gingivales superiores, for gums and sockets. The teeth of the lower jaw innervate the lower alveolar nerve, item alveolaris inferior, the branches of which form the lower dental plexus, plexus dentalis inferior.
Root made of dentin and cellulose with a cement coating that anchors the tooth to the jaw. The root is especially vulnerable to injury and infection because it lacks protective enamel. Tooth root infections can spread into the bloodstream or the surrounding jaws and tissues, so tooth root infections require prompt and thorough medical care... A crown, consisting of a thick enamelled surface that is used for cutting and chopping food. A thick layer of dentin lies under the enamel, between it and the dental pulp.
- The neck, which is the place where the cementum of the root meets the enamel of the crown of the tooth.
- The root has thin layer enamel and a thick layer of dentin that protects the root.
The dental plexus gives off the lower dental branches, rami dentales inferiores, to the teeth and the lower gingival branches, rami gingivales inferiores, to the gums and walls of the holes. The dental nerves, together with the vessels, pass through the apical foramen into the tooth cavity, branching into the tooth tissues.
4. MODERN METHODS OF RESEARCHING HUMAN TEETH
The main methods for studying teeth are odontoscopy and odontometry, which are carried out on native preparations, jaw models and radiographs. Odontoscopy is a visual study and description of the structural features of an organ. The tooth is viewed in various positions.
To prevent potentially dangerous ingestion of the tooth root. To prevent bacteria from entering the enamel of the neck and crown of the tooth. To prevent the spread of infection from the tooth to other parts of the body. All of the above. Both A and B are the reasons why dental floss important for maintaining the health of the teeth as well as the body.
Most likely an animal's diet with sharp, sharp incisors in the front of the mouth and flat, crumbling molars in the back? Carnivorous diet with meat. An omnivorous diet with plants and meat. Herbivorous plant diet. None of the above. An animal that has incisors and molars but no canines is probably herbivore.
The description of the tooth in the medical and anthropological literature begins with the vestibular norm, then characterizes the tooth in lingual, occlusal, approximal norms.
Odontoscopy is completed by examining the tooth cavity. V orthopedic dentistry Special attention devoted to the anatomy of the tooth crown. When describing a tooth, they give a characteristic of the contours of the tooth and the relief of its surfaces.
Which one of possible consequences injuries or infections of the teeth of a wild animal? The infection can spread to other parts of the body, which can lead to death. The animal may not be able to ingest enough nutrients to survive.
Upper and lower jaw. Anatomical features important for dental prosthetics
In some. The tooth is one of the most individual and complex anatomical and histological structures in the body. The composition of the tooth tissue is located only inside the oral cavity and is limited to the dental structures. Each tooth connects in the same jaw, and the opposing jaws have teeth that are classified within the same category, however, they are not grouped according to structure, but function. They are located within the upper and lower alveolar bones in the lower and lower jaws, respectively, and this exclusive type of joint is known as gomphosis.
A tooth that occupies the same position with respect to the tooth on the opposite side of the dental arch (antimer) has structural features that make it possible to determine its belonging to one of the sides (lateralization of the tooth). The main signs of lateralization are the sign of crown angle, sign of crown curvature and sign of root position.
Characteristics of some pathological processes
Recommended video: Tooth Anatomy. The structure of the tooth seen at the intersection. The teeth are divided into four quadrants within the mouth, with the separation occurring between the upper and lower jaws horizontally and along the midline of the face vertically. This leaves up to eight adult teeth in each quadrant and separates opposite pairs within the same alveolar bone, as well as their counterparts in the opposite jaw. Each quadrant contains a medial and lateral incisor, a canine, two premolars, and two to three molars.
The traditional anatomical approach to the description of teeth involves determining the belonging of a tooth to its generation (milk or permanent), class (incisor, canine, premolar, molar), side of the dental arch (left, right) and odontoscopy in various rates (vestibular, lingual, medial and distal).
Each of the standards requires the following characteristics: the shape of the structures: the shape of the surfaces of the crown, the shape of the tubercles of the occlusal surface, the curvature of the root (s); the number of morphological formations (enamel ridges of the vestibular surface, tubercles of the chewing surface); “Qualitative features of the structures (splitting of the tubercle, the presence or absence of enamel streaks); the spatial location of the formations (localization of the tubercles of the occlusal surface, the direction of the grooves of the occlusal surface, the position of the scallops, the direction of the convexity of the enamel-cement border); »The mutual arrangement of structures (the relation to each other of the marginal ridges, tubercles of the occlusal surface, roots in multi-rooted teeth); the magnitude or severity of morphological structures (enamel leakage).
Incisors are used for cutting and biting, canines are used for gripping, and premolars and molars are used for comminution. The main functions of teeth include chewing food in a bolus that can be swallowed easily for further digestion, giving structure, support and shape to the tissue in the face and helping to make sounds during speech.
A tooth consists of a crown and one or more roots. The anterior teeth in both the upper and lower jaws, from the right first premolar to the left first premolar, are single root teeth. On the upper jaw, the maxillary second premolar may have two roots, and all maxillary molars have two or three roots. In the lower jaw, the premolarium of the lower jaw has one root, and the molars have one or two roots.
The description of the tooth is given, starting with the vestibular norm, taking into account that in the oral cavity the tooth faces the researcher with the vestibular surface.
After describing the vestibular norm, it is advisable to characterize the lingual surface. The third position is the occlusal norm, which describes the working surface of the tooth. Further, the medial and distal surfaces are characterized by comparing them with each other.
The articulating surfaces at the very top of the crown of the teeth are designed to function as a tooth, so the front teeth, from the right canine to the left ear, have one sharp edge that can pinch and break while premolars and molars have splinters, pits and cracks that able to grind and bake a sip of food to make it edible.
Types and functions of teeth
The crown of the tooth is the visible part of the tooth in the mouth, while the root is hidden under the gum and alveolar bone. It has a pearly white up yellow color depending on the thickness of the enamel, the age of the patient, their oral hygiene and lifestyle choices. Enamel is the outer layer of a tooth that is extremely strong and durable. Underneath this tough appearance there is a second softer layer that is slightly darker in color and is known as dentin. It is a capsule that separates the hard outer tissue from the soft and fragile pulp cavity, which is the innermost layer of the tooth and contains the blood vessels and nerves of the tooth.
When odontoscopy, in each of the norms, the crown and root of the tooth are considered, the contours of which are compared in shape with geometric shapes (triangle, trapezoid, square, rectangle, rhombus, oval).
Comparison with geometric shapes is convenient for characterizing general patterns of tooth structure. In odontoscopy, the features of the transition of the contours of the crown to the corresponding contours of the root are described.
In this case, the nature of the transition of the contours of the crown and root at the surfaces located opposite each other is compared. Each of the standards describes the shape and spatial arrangement of the enamel-cement border.
An important odontoscopic assessment is the description of the surface topography. At the same time, the presence of protruding areas on the crown (enamel ridges, ridges, tubercles), depressions (grooves, pits) on the crown and root are indicated. For the topical characteristics of the morphological formations of the tooth, the crown and root are divided into conditional parts.
On the vertical axis in the vestibular, lingual, medial and distal norms, the crown is divided into occlusal, middle and cervical thirds, and the root - into cervical, middle and apical thirds.
Along the frontal axis in the vestibular and lingual norms, the medial and distal half are isolated in the crown.
Along the sagittal axis in the medial and distal norms, the crown is divided into the vestibular and lingual parts.
The study of the tooth is completed by characterizing its cavity using thin sections made in two mutually perpendicular projections (in the vestibular-lingual and myial-distal), as well as by radiographs. Describe the ratio of the tooth cavity to its external shape.
The localization of the mouth of the canal (s) at the bottom of the crown cavity, the width of the lumen are indicated, and in multi-rooted teeth they give comparative characteristics channels (mark the channel of the largest diameter, narrowing in various cavities, curvature, branching).
The topography and size of the opening (s) of the root apex are noted. An objective method for studying teeth is odontometry, which is understood as a set of methods for measuring a tooth. For odontometry, a vernier caliper with pointed legs is used, which allows measurements to be made with an accuracy of OD mm.
To unify measurements on the surfaces of the tooth, it is necessary to apply the following guidelines with a pencil: - the border of the crown base and root; - the projection of the conditional median vertical of the tooth.
The border of the base of the crown (root) connects along the perimeter the points of the greatest convexity of the enamel-cement border on the vestibular and lingual surfaces of the tooth.
The projection of the conditional median vertical is depicted on the medial, distal, vestibular and lingual surfaces of the tooth. To do this, perpendiculars are restored on both sides of the midpoint of the border of the crown and root.
The most important odontometric parameters are: tooth height, height (length) of the root (s), crown height, vestibular-lingual size (diameter) of the crown, vestibular-lingual size (diameter) of the neck, medial-distal size (diameter) of the crown, medial-distal size (diameter) of the neck, the severity of the curvature of the enamel-cement border.
Tooth height is defined as the distance between the outermost points of the crown and root.
The height (length) of the root must be measured in the medial (or distal) norm, focusing on the border of the base of the crown (root) and the apex of the tooth root.
The height of the crown of a tooth is determined by the difference between the height of the tooth and the height of the root. The vestibular-lingual size of the tooth crown is the distance between the largest protuberances of the vestibular and lingual surfaces.
The vestibular-lingual neck size is determined between the points of the greatest bulge of the enamel-cement border of the vestibular and lingual surfaces. The medial-distal crown size is measured between the outermost (contact) points of the proximal surfaces.
The medial-distal size of the neck is determined between the points located at the intersection of the enamel-cement border and the projection of the conditional median vertical on the medial and distal surfaces of the tooth. The severity of the curvature of the enamel-cement border is determined in medial and distal rates as the shortest distance from the point of its greatest convexity to the level of the crown base.
In dentistry they use X-ray methods examinations including intra- and extraoral radiography, tomography, panoramic radiography and orthopantomography. The most informative method X-ray examination teeth is orhopanthography.
The method consists in the passage of X-rays perpendicular to the axis of the tooth throughout the entire alveolar process of the jaw. This method research allows you to establish the number of teeth, their relative position and the presence of damage to the tissues of the tooth.
The hard parts of the tooth and the surrounding bones trap X-rays; as a result, the contours of the tooth, its cavity, surrounding tissues and the relationship of teeth with other structures are clearly visible on the film. The enamel of the tooth creates a dense shadow and contrasts with cement and dentin, which allows you to define the boundary between the base of the crowns and the root.
Dentin and cementum are not differentiated on the radiograph. The tooth cavity is recognized by the outline of the dentine contour, because the pulp does not retain X-rays. The cavity of the crown is defined as a vacuum with clear contours; root canals, tapering from the cavity of the crown to the apex of the root, repeat the bends of the root.
The gap between the cement of the root and the alveolus in the form of a uniform dark stripe corresponds to the periodontal gap. In children, on radiographs in the area of the roots of the milk teeth, the rudiments of their replacement permanent teeth are located on different stages development.
Permanent teeth are located under the milk teeth in a capsule, which is revealed in the form of enlightenment. In the distal regions behind the milk molars, additional teeth are formed - permanent bite molars. In the X-ray image, milk teeth differ from permanent ones in their smaller size and shape. Permanent teeth are located in the dentition and are separated from each other by an interdental septum.
Interdental septa are represented by cancellous bone, bordered along the periphery by a clearly defined closing cortical plate of the alveoli. The maxillary medial incisors come close to the cancellous palate and to the bottom of the nasal cavity. The root of the lateral incisor is somewhat distant from the nasal cavity.
On intraoral radiographs of the anterior part of the upper jaw, in the middle of the interdental septum between the medial incisors, the clearing band of the intermaxillary suture is determined.
At the level of the tops of the roots of the medial incisors, an incisal opening is revealed in the form of an oval focus of enlightenment. The apex of the canine root of the upper jaw reaches the bottom of the nasal cavity near the nasal notch. The roots of premolars and molars are located near the maxillary sinus.
At the level of the tops of the premolars, there is a noticeably smooth or tuberous bony eminence - the palatine torus. The molar roots sometimes protrude into the cavity maxillary sinus and covered only with mucous membranes. The medial incisors of the lower jaw are located on either side of the intermaxillary suture, which is determined before the age of 1 year.
On the lingual surface of the lower jaw, according to the roots of the canine and premolars, sometimes a smooth or bumpy bone formation... At the level of the tops of the roots of the premolars, an oval focus of enlightenment is determined, corresponding to the position of the chin foramen.
Below the roots of the molars, a focus of rarefaction of bone tissue with fuzzy contours is sometimes determined - the submandibular fossa.
The canal of the lower jaw in the form of a strip of bone tissue rarefaction is located close to the roots permanent molars, especially the first.
5. DEVELOPMENT AND ANOMALIES OF DEVELOPMENT OF TEETH
5.1. Comparative anatomy teeth
In evolutionary terms, teeth are a derivative of ectodermal epithelium, transformed into scales. The scales of ancient fish, which were on the jaws, gradually underwent significant development and gave rise to teeth.
The simplest form of teeth is conical. In lower vertebrates, conical teeth are very small, but numerous (sometimes thousands). They are all the same in shape (homodont system).
In more highly organized animals, in particular in mammals, teeth of various shapes (heterodontic system) have formed, which are functionally adapted to the animal's diet.
The base of the teeth in most vertebrates is fixed to the underlying jaw using connective tissue.
On the jaws of different classes of animals, teeth can be strengthened in different ways: along the edge of the jaw (acrodontic teeth), the outer dental edge to the inner edge of the jaw (pleurodont teeth), in special cells of the jaws (thecodont teeth).
The latter type of teeth originated in fossil reptiles. The teeth of the ancient lower vertebrates were temporary and replaced like the scales of a keratinizing multilayer squamous epithelium... As they wear out, they were replaced by new ones (polyphiodont type).
In the process of the evolutionary development of organisms, the number of tooth changes decreased, and in modern mammals, as well as in humans, there is only one tooth change (diodont type).
In the process of evolution, the fact of tooth reduction is noted. One of the first changes in the dental system was the reduction in the size of the canines and the closure of the diastemas. The second stage in the evolution of the dental system was mediolateral reduction of molars and the transition of the main functional role from the 2nd to the 1st molar.
Subsequently, there was a decrease in the size of all teeth. Compared to primates, humans are characterized by a decrease in the size of the teeth, due to the weakening of the chewing apparatus. There are also signs of reduction of the last large molars (incomplete eruption, underdevelopment, absence).
5.2. Teeth development
Teeth are derived from the mucous membrane oral cavity... From the epithelium of the mucous membrane, enamel organs develop, and from the mesenchyme located under the epithelium - dentin, pulp, cement, the surrounding tooth - hard and soft tissues (periodontium).
The development of teeth goes through three stages: in the first, the bookmarks of the teeth are formed, in the second, differentiation of the tooth germs occurs, and in the third, the formation of teeth.
In the first stage, at the 6-7th week of intrauterine development, a thickening of the epithelium occurs on the upper and lower surfaces of the oral cavity - dental plates, on which flask-shaped protrusions are formed, which then turn into the enamel organs of milk teeth.
At the 10th week of embryogenesis, the mesenchyme grows into the enamel organs, which is the rudiment of the dental papillae. By the end of the 3rd month of development, the enamel organs separate from the dental plates, being in conjunction with them through epithelial tissues - the neck of the enamel organ.
Due to the compaction of the surrounding mesenchyme, a dental pouch is formed, which merges with the dental papilla. In the second stage of tooth development, the homogeneous cells of the enamel organ are divided into separate layers.
In the center, a pulp is formed, and on the periphery - a layer of internal enamel cells, giving rise to ameloblasts participating in the formation of enamel. Simultaneously with the transformation of the enamel organ, differentiation of the dental papilla occurs. It increases in size and grows deeper into the enamel organ. Vessels and nerves approach the papilla.
On the surface of the papilla, odontoblasts - dentin-forming cells - are formed from mesenchymal cells. By the end of the 3rd month, mesenchyme grows in the cervix, they dissolve, and the tooth buds separate from the dental plate.
Persist and grow back sections and the free edges of the dental plates, which are further transformed into the enamel organs of the permanent teeth. Bone beams grow around the tooth buds in the jaw mesenchyme, which form the walls of the dental alveoli.
In the third stage of dental development, starting from the 4th month of the prenatal period, dental tissues appear - dentin, enamel and dental pulp. Due to odontoblasts, dentin is formed, which begins to calcify at the end of the 5th month.
At the apex of the dental papilla, ameloblasts begin to form enamel. In the future, enamel calcification occurs, which ends only after teething. In this case, the calcification of the crowns first occurs, and then the roots of the teeth. Due to the formation of a tooth crown upper section the enamel organ is reduced.
The lower section turns into an epithelial sheath containing mesenchymal cells. They become odontoblasts that form the dentin of the tooth root. The development of the tooth root takes place in the postembryonic period. The mesenchymal cells of the dental sac are converted into cementoblasts, which produce cement on the surface of the dentin of the tooth root.
The pulp develops from the mesenchyme of the dental papillae. Permanent teeth also arise from dental plates. At the 5th month of development, the enamel organs of incisors, canines and small molars are formed behind the rudiments of milk teeth.
At the same time, the dental plates grow posteriorly, where the enamel organs of the large molars are laid along their edges.
Further stages of formation are similar to those described for milk teeth, and the rudiments of permanent teeth lie together with the milk tooth in one bony alveolus.
The rudiments of permanent teeth begin to calcify in the first months after birth. First, the first molars are calcified, then the premolars, canines and incisors. At three years old, the second and third large molars remain uncharged.
Calcification of the roots of permanent teeth is completed only by 15 years, and the roots of wisdom teeth - by 25 years. 5.3. Tooth abnormalities The term "abnormality" means a deviation from the norm. Tooth anomalies include anomalies of their shape, size, structure, color, quantity, position in the dentition, timing of eruption.
During the period of the establishment and formation of tooth germs, deviations in the direction of their increase or decrease are possible, which leads to anomalies in the number of teeth: hyperodentia, hypodentia or complete adentia of primary and permanent teeth. Hyperdensity or an increase in the number of teeth is observed more often in the frontal region, less often in the area of premolars and molars.
Supernumerary teeth can be normally developed, have the correct shape and be located in the dentition, practically without causing disturbances. Between the medial incisors on the upper jaw, an additional tooth is sometimes found - the meziodens, mesiodens, which has a peg-shaped shape and does not reach the level of the incisal edge of the adjacent medial incisors in height.
An increase in the number of teeth is more often expressed by the appearance of an additional 3rd upper incisor, or 3rd premolar, or 4th molar.
Supernumerary teeth usually develop outside the dental arch. Much more often supernumerary teeth have shape anomalies, complicate the eruption of complete teeth, lead to anomalies in the shape of the dentition and occlusion.
An increase in the number of tooth buds can cause a hard odontoma. Simple odontomas associated with enamel are called enamel drops. Complex odontomas consist of a large number teeth, among which there may be normally formed teeth.
Hypodentia is a decrease in the number of teeth. Its origin is due to the phylogenetic reduction in the number of teeth in humans. The most common cases are edentulous third molars, second premolars and permanent lateral incisors. Edentulousness of other teeth is less common.
Hypodentia can be a sign of such hereditary diseases as anhydrotic dysplasia (Christ-Siemens-Turner syndrome), chondroectodermal dysplasia and is often associated with clefts of the lip and palate.
A decrease in the number of teeth leads to anomalies in the dentition and occlusion and, as a rule, adversely affects the functioning digestive system and mental activity child.
With primary adentia, underdevelopment of the alveolar process of the upper jaw or the alveolar part of the lower jaw is noted. The diagnosis of adentia is made on the basis of anamnestic data and results of an x-ray examination.
Most often, the last molars are absent, the upper lateral incisor or fang. Sometimes the rudiments of ten teeth or more are missing. Complete adentia is extremely rare.
With adentia of the lateral incisors of the upper jaw, there are gaps between the teeth - diastemas and tremes,
Often there is non-eruption - retention of teeth, when their rudiments remain hidden in the jaw. This may be due to impaired growth of the jaw or premature extraction of milk teeth.
If the growth of the jaw is disturbed, the roots of adjacent teeth are fused, which is the reason for retention. At early removal a canine or upper molar of a milk bite, an overgrowth of the alveoli may occur bone tissue and moving the first premolar or first permanent bite molar to the location where the adjacent tooth is to be erupted.
Retention is more common in the canines of the upper jaw, third molars of the lower jaw, and less often in premolars. Anomalies in the position of the teeth are very common and can be very diverse.
The most common abnormalities are the displacement of one or more teeth from the dentition towards the palate or in the vestibule of the oral cavity.
Less commonly, there is a 90 ° rotation of the tooth (tarsia) around its axis or change of teeth in places (transposition). In the latter case, for example, a premolar grows in place of the canine and vice versa.
The teeth can slide over each other, i.e. their crowding occurs.
Sometimes, during eruption, there is a movement of the tooth bookmark from the dentition to solid sky, nasal cavity, maxillary sinus, anterior wall or tubercle of the upper jaw.
Such movements are called heterotopia of teeth. Teeth that have erupted at the time of birth are called neonatal. Early teething is quite common.
There are known cases of intrauterine eruption of the central milk incisors of the lower and less often of the upper jaws. The reasons for this may be the accelerated development of the tooth germ, its superficial location or inflammatory process periosteum of the jaw or gums.
The crowns of premature teeth are usually smaller in size, yellowish in color, with areas of enamel necrosis. In order to preserve breastfeeding, congenital teeth are removed in most cases. Since the root of the tooth develops later, the removal of the crown is easy.
However, in the area of the removed crown, a root of a smaller size may develop in comparison with the usual one. The germ of the same name permanent tooth develops normally, but more often in more early dates... Late teething is also very common.
It is caused by endocrinopathies, hereditary diseases, diseases of the digestive system and nutritional disorders. Anomalies in the size of teeth include macro- and microdengia.
With macrodentia, the medio-distal dimensions of the teeth significantly exceed the average. Giant central upper incisors sometimes exceed the width of both lower incisors. Less commonly, giant teeth are found among the lower incisors and premolars.
Macrodentia can affect both permanent and milk teeth. Microdentia is characterized by a decrease in the size of the teeth, often combined with anomalies in the dentition and with the appearance of diastemas and three.
The teeth located in the distal regions of each class and, in particular, the lateral incisors of the upper jaw, are most susceptible to reduction.
Normally, the ratio between the medio-distal dimensions of the medial and lateral incisors is 1: 0.8. At the first degree of reduction, the mediodistal size of the crown of the lateral incisor is about half that of the medial incisor of the upper jaw.
With the second degree of reduction, the lateral incisor has a conical shape, but the height of its crown is normal. With the third degree of reduction, the lateral incisor of the upper jaw does not exceed half of its normal height.
In case of disturbances in the formation and differentiation of tooth rudiments, teeth of an irregular shape are formed. There are abnormalities in the shape of the crown, root or tooth as a whole.
Among the variety of anomalies in the shape of teeth, some have a characteristic clinical picture, by which it is possible to judge the origin of the anomalies (teeth of Hutchinson, Fournier and Pfluger in congenital syphilis).
Anomalies in the shape of the tooth are very diverse. These include subulate, conical, cuboid, screwdriver,< бочкообразные формы резцов. Аномалии формы больших и малых коренных зубов проявляются изменениями количества бугорков и степенью выраженности рельефа жевательной поверхности. Весьма многообразны аномалии корня.
These are curvature, twisting, splitting, accretion, change in the number, size and shape of the roots. Root accretion is more common in the anterior adjacent teeth.
There are several types of teeth fusion: crowns, crowns and roots, if any separate cavities tooth, complete fusion of two adjacent teeth to form a single tooth cavity. Developmental abnormalities can only affect the roots of the teeth.
An increase in the number of roots is most often noted, for example, roots of incisors, canines and premolars can develop. So, premolars can have not only two, but also three roots, and in molars, their number reaches five. There may also be a decrease in the number of roots in multi-rooted teeth. The most common root fusion is observed in wisdom teeth.
Extremely pronounced curvature of the roots most often affects the canines, premolars and the last molars. In the process of histogenesis, there may be disorders associated with the formation of dentin, enamel, cement, tooth pulp and periodontal tissues. Anomaly of dentin development - imperfect dentinogenesis.
With this pathology, both milk and permanent teeth have amber translucency, the enamel easily breaks off, which contributes to the erasure of exposed dentine.
Imperfect amelogenesis is caused by impaired enamel development and is known under various names: hereditary enamel hypoplasia, enamel aplasia, brown enamel, brown dystrophy, corrugated teeth.
All malformations of enamel can be attributed to the following groups: insufficient enamel formation (hypoplasia), insufficiency of primary calcification of the organic matrix (hypocalcification), defects in the formation of hydroxyapatite crystals in various parts of the enamel (hypo maturation), deposition of exogenous material, often of a pigmented nature, and combinations these violations.
The combination of impaired amelogenesis and denginogenesis is expressed in Stanton-Candepone syndrome. The color of the teeth in this syndrome is watery-gray, sometimes with a brown tint.
Soon after the eruption of the tooth, the enamel is chipped off due to the fragile connection with the dentin. The roots of the teeth can be shortened and thin or, conversely, thickened.
Teeth are our tools that carry out the primary mechanical processing of food. Since ancient times, the presence healthy teeth meant a higher ability to survive, since the loss of the ability to chew hard and rough food could threaten with starvation.
The anatomy of the tooth tells us that this is a formation of tissues special for their function, which have their own nervous and circulatory apparatus. Normal teeth should be between 28 and 32. Alas, without outside interference, they are replaced only once in a lifetime, when molars are erupting instead of falling milk teeth.
Anatomy of the teeth of the upper and lower jaw
Dental buds are formed in the fetus already in first trimester of pregnancy, during the 7th week of development. At the same time, in place of the future alveolar processes epithelial tissue thickens and, forming a symmetrical arc, grows in the depth of the mesenchyme. Subsequently, perpendicular secondary plates are formed under it.
In tooth buds, meanwhile, from epithelial cells begins to form tooth enamel ... With the growth of the dental plate, the enamel organs appear in front and separate from it. It is then that the constituent parts of the future tooth are formed.
What we see when we smile is just a crown of a tooth
At normal anatomy teeth in humans, the epithelium is converted into enamel, and the mesenchymal tissue forms dentin and pulp, a cement sheath appears that protects the tooth root (see photo). The rudiments themselves remain in the alveolar processes. waiting for its teething time.
According to their structural parts teeth are usually subdivided into crown, neck and root:
- crown- this is the visible part, which is located above the gum and is directly involved in grinding food;
- neck- this is the part located inside the gum, not covered with enamel, but protected with cement;
- root it is hidden in the alveolus, connecting the teeth with the bone tissue of the jaw, and through the canal of which nerves and blood vessels run into the cavity of the tooth.
The cavity itself is filled soft cloth, penetrated by many nerve and vascular endings, and is called the pulp.
The main part of the dental tissue consists of dentin which is located around the pulp and is protected from damage tooth enamel on the crown and cement in the area of the neck and root.
Types of teeth
Human teeth differ from each other in their function and location. But despite this, anatomical structure teeth of the upper and lower jaw are characterized by a similar principle of growth and the same internal structure. In total, an adult should normally have from 14 to 16 on each jaw.
Every tooth can be seen from six positions... From below, it goes roots into the gum, on both sides it comes into contact with neighbors (if any), with one side facing the cheek or lips, the other toward the tongue.
Another plane to consider is the chewing plane. It touches the same surface of the other jaw's tooth every time the person squeezes them.
Inside the tooth contains a pulp - a cavity with blood vessels and nerves
Each tooth in the dentition has its own antagonist... For example, the 6th tooth of the lower jaw, when chewing, comes into contact with the 6th tooth of the upper jaw. This allows food to be grinded and prevents the roots from gradually coming out of the alveoli without pressure on the crown. In addition, it forms the correct bite, which is important for the health of the oral cavity.
First of all, a person has incisors. They got this name because with their help they bite off (cut) the necessary share of food for further processing.
This is facilitated by their shape resembling a chisel. In the incisors, especially the upper ones, the crown is much wider in front and behind than on the side.
As a rule, the roots and root canals of the incisors are one at a time. The central incisors are usually larger than the lateral ones. The crown, however, is not perfectly flat, but rather bumpy, which makes it easier to "saw off" the desired size piece of food.
The incisors are slightly concave with inside and rounded on the outside. The roots in this case are rather long and have a conical shape.
Next come fangs. There are only 4 of them - 2 at the top and 2 at the bottom. Their roots are also single and longer than the coronal part, but not as long as those of the incisors. Unlike incisors, their cutting edge is not so long and it can be divided into two halves, distal and mesial, which converge in the form of an angle.
The canine of the upper jaw is wider by the size of the crown than its antagonist on the lower one. It is convex from the outside, and slightly concave inside.
Then there are small molars, or as they are also called - premolars. There are 8 of them in total, that is, on each half of the upper or lower dentition there are 2 pieces - mesial and distal. The roots in the premolars are usually one to two. On the distal, the chewing surface is sharper, on the mesial it is flatter and more extended.
In total, an adult has from 28 to 32 teeth
The first premolars are often canine-like., since they have a sloping outer edge and a pronounced sharp edge. On the lower jaw, the small molars are smaller in size, especially the first. The second premolars are more intended for chewing.... They have a larger crown, which often has four sides.
Large molars are also called molars... Depending on whether the third molars have erupted, their number varies from 8 to 12. The coronal part of the molar looks like a cube. However, its edges are not perfectly flat. There are several bumps on the chewing surface that help to effectively grind food during the meal.
Above, large molars usually have three roots, while the lower 7th tooth, like the 6th, has no more than two roots. Six, that is, the first of the large indigenous people probably has the largest crown of all teeth especially on the upper jaw. The next seven is slightly smaller in size, and it is subjected to less stress when chewing.
Third molars
As for the third molars, there are often from three to four roots, and they can intertwine into one large cone-shaped root, so even with an X-ray it can be difficult to tell how the roots of teeth look in the eighth position.
In some cases, the eruption of the third molar does not lead to any complications, pain or inflammation. However, sometimes the growth of the figure eight and its further presence in the mouth causes suffering..

The roots of the tooth contain a root canal through which vessels and nerves pass into the pulp
In case of such complications, you should contact your dentist. who will most likely send you an X-ray and give you advice on further action... It may be necessary to slightly cut the gums to facilitate the emergence of a wisdom tooth. Otherwise, it is likely that it will grow crooked or cause inflammation of the mucous membrane.
In some cases, the third molar may be better removed.... Grown incorrectly, in the "backyard" of the jaw, it will be quite difficult to clean and often accumulated infection can cause tooth decay, gum inflammation and even infection. Such a collector of microbes can cause serious harm the whole mouth and it is not known what diseases can still develop due to this.
Another reason for removal may be the uselessness of the figure eight in the process of primary processing of food. In most cases, the wisdom tooth is not involved in chewing in any way, and if it is clear that it is clearly not healthy, then you should start removing it as early as possible.