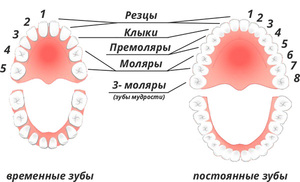
Diagram of the dental arch of permanent dentition
An adult has only 32 teeth in his permanent dentition, but this is normal. There are 16 teeth on each jaw. There are 4 types: incisors, canines, premolars and molars. The incisors, in turn, are divided into central and lateral. But what kind of teeth are molars? These are the ones that help us chew food thoroughly.
In total there are 8 incisors, 4 canines, 8 premolars and 12 molars. There are 3 molars on each side of the jaw. But this is all normal. Often 3 molars do not erupt or 1 or 2 units appear.
Molars and premolars are commonly referred to as molars and molars. Thanks to them, food is thoroughly grinded and very hard products are crushed. Premolars are very similar to their “big brothers”, large molars. They are quite capable of performing all functions in the event of loss of molars. However, there are certain differences in their structure. There are first and second lower premolars, as well as upper ones. Between themselves they also have differences in anatomical structure.
Anatomy of the upper premolars
These units are prismatic in shape. In size they can be from 19mm to 25mm. Most often their length is 23mm. On upper jaw, they are usually slightly larger than on the bottom.
The chewing surface of such teeth is made of 2 tubercles, buccal and palatal. Between them there is a shallow groove - fissure. The buccal tubercle is slightly larger than the palatine tubercle.
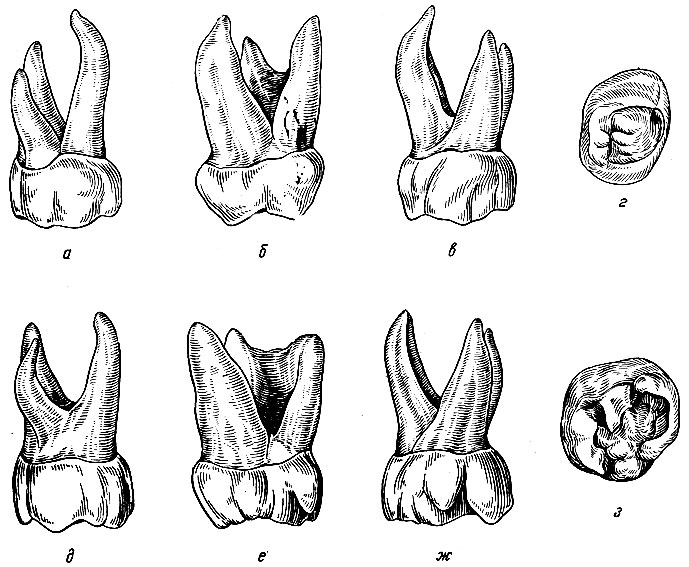
The first premolar has 2 roots, which are located closer to the oral and vestibular surfaces relative to the crown. More often they are direct, with good channels. Closer to the top, the roots may have a slight bend. The second premolar is very similar in structure to its “neighbor” predecessor. However, it has one large straight root, with a wide channel.
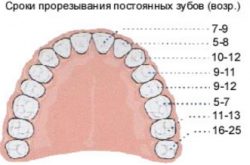
 Timing of teeth eruption on the upper and lower jaw
Timing of teeth eruption on the upper and lower jaw
Anatomy of lower premolars
The first lower low-rooted tooth is very similar in appearance on the fang. But upon closer examination, 2 tubercles are also found on its chewing surface, with the same location as on the upper jaw. However, the lingual cusps are not very pronounced. On both units of the lower jaw, the premolars have one root, slightly compressed in the medio-distal direction.
These teeth are already permanent. The first premolars erupt only at the age of 10, and the second a little later at the age of 13. But what is more interesting about molars is what kind of teeth and what do they look like?
Large molars - their functions and structure
If we consider the norm, then there are 12 molars in total, six on the upper and six on the lower jaw, 3 units on each side. They are located last in the dental arch, for this reason the term “posterior” teeth is often applied to them.
Their main function, chewing food. For this purpose, nature provided to make them the largest. Moreover, they also have the largest chewing surface. Under conditions of sufficiently strong enamel, molars can withstand loads of up to 70-75 kg. So, molars are what kind of teeth?
Large teeth of the upper jaw
 Maxillary molars
Maxillary molars They are really big, but not much bigger than the ones below. On the chewing surface there are 4 tubercles separated by transverse grooves. The mounds are small in size. The size of the coronal part is 6.5 – 9.0 mm.
From the crown, 3 roots extend into the alveolar process: one palatal and 2 buccal, medial and distal. The buccal-medial root is slightly larger and longer than the others. They are usually straight, with fairly wide channels. In some cases, the second molar even has 4 roots. This happens in about 10% of cases. In terms of the shape of the crown, it is quite similar to the first unit.
Most wisdom teeth are somewhat smaller than other chewing units, only in in rare cases they can be abnormally large. In certain cases they are completely absent, and today this is not considered to be any serious anomaly. Scientists believe that such things became unnecessary in the process of human evolution. Large quantity chewing teeth, was necessary when a person consumed solid food. Today, thanks to the benefits of civilization, it has become possible to prepare softer food, which does not require the effort of grinding it to the desired consistency. Therefore, nature decided that such teeth are no longer in demand.
Third molars have three cusps on the chewing surface, in rare cases 2 or 4. Root system represented by 3 units. The roots are most often fused together, curved, with poor passable channels. Therefore, they cannot be treated if they are affected by pulpitis or periodontitis. There is evidence that wisdom teeth have up to 5 roots. 
Third molars usually always cause problems. They are difficult to erupt and provoke inflammatory processes in the gums, their location in the dental arch is often incorrect. The 4th molar is very rare. This is certainly an anomaly. Such units are completely underdeveloped and must almost always be removed.
Lower large chewing teeth
These units are somewhat smaller than those on the upper jaw. The 1st and 2nd molars have an almost identical structure. On the chewing surface of the first there can be from 3 to 6 tubercles. The second molar is represented by 4 cusps, quite well defined in structure. Sometimes there can be 5 of them.
 Topography of molars on the lower jaw
Topography of molars on the lower jaw Both teeth have 2 roots that follow each other (medial and distal). The roots are thinner than the upper “brothers” and also have narrower root canals.
Eights are most often underdeveloped. They may not fully erupt and be partially covered by the gum mucosa. The wisdom teeth on the lower jaw have one massive root, less often there are 2 units, but they often grow together. Root canals, strongly curved and not amenable to endodontic treatment. Its displacement in the medio-distal direction or in the buccal direction is often observed.
They erupt quite painfully. All this is often accompanied by a rise in body temperature, malaise, refusal to eat and painful tearing of the mouth. Children have 2 primary molar units. The first ones erupt from 12-14 months, the second ones appear from 20-24 months.
Primary molars are almost a copy permanent teeth. However, their crowns have more pronounced cusps and deepened fissures, which contributes to the development of carisogenic processes. Their roots are also highly branched and slightly curved.
When the time comes to change the bite, the roots begin to dissolve - they are resorbed. First permanent molars appear already at 6-7 years of age. The second ones are a little later than 12-13 years old, and wisdom teeth at 21 years old and even at a later age.
The question of molars is what kind of teeth parents often ask of those children whose bite is changing or only milk teeth are just erupting. In this case, it is important for parents to at least approximately remember the timing of teething, both permanent and baby teeth, and in case of any problems or suspicions, be sure to consult a doctor. Early detection problems with the formation of the dental arch will help to avoid more in the future.
If you have any questions after reading the article, we are always happy to answer them in the comments.
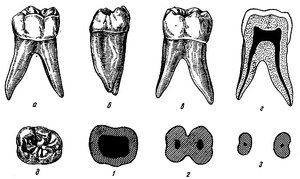
Large molars (molars)(dentes molares). There are 12 large molars: 6 upper and 6 lower, 3 on each side of the dental arch. There are 1st, 2nd and 3rd ( wisdom tooth, dens serotinus) molars. Large molars have the largest crown, an extensive occlusal surface (with 3-5 cusps), and several roots. They play an important role in chewing (molares - millstone). Molars are located in the dental arch behind the premolars, which is why they are called posterior teeth.
The size of large molars gradually decreases from the 1st to the 3rd. When chewing, the molars have a lot of pressure heavy load(the average load on the 1st molar is 77 kg, on the canine and premolar - from 20 to 40 kg).
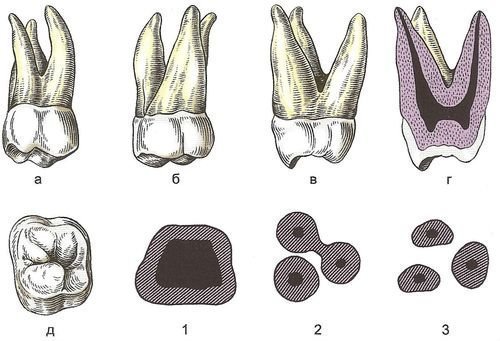
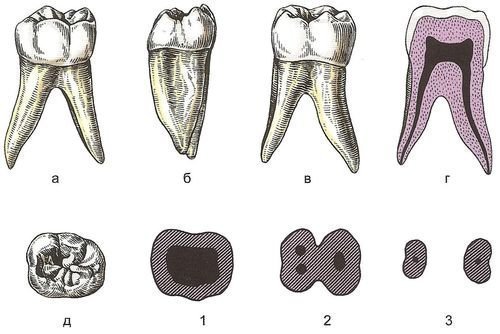
Upper molars. These teeth are slightly larger than the lower molars. The occlusal surface of the crown of the upper molars is rhombic in shape with rounded corners, divided by 3 grooves (in the shape of the letter H) into 4 cusps. The teeth have 3 roots (rarely 4): a rounded lingual and 2 cheek, flattened. The 3rd molar (wisdom tooth) is variable and slightly smaller than the others.
1st upper molar has a crown similar to a rectangular prism, the corners of which are rounded (Fig. 1). The buccal surface of the crown is quadrangular with a longitudinal median sulcus, the severity of the groove varies from a small groove at the cutting edge to a deep groove dividing the crown into two halves - mesial and distal. The groove sometimes continues to the initial part of the root, where it widens and deepens due to the presence of two buccal roots. On the cutting edge there are two high triangular tubercles: mesial and distal. The mesial tubercle is usually higher than the distal one.
Rice. 1. First upper molar, right:
At the base of the crown in its cervical third there is an elevation - a belt (cingulum). The development of the belt is different: from a weakly expressed to a very clearly defined ridge. Enamel-cementum junction on the buccal surface of the tooth is straight or slightly curved, convex to the root. Sometimes an interradicular leak of enamel develops from a small triangular protrusion to a wide strip of enamel extending deep between the roots and corresponding to the buccal median sulcus. The contact surfaces of the crown converge slightly towards the neck and form bends with the lateral surfaces of the roots. The distal curve is less than the mesial one.
The occlusal surface is large, diamond-shaped or square. There are 4 tubercles on it: buccal-mesial, buccal-distal, lingual-mesial and lingual-distal. The most developed and resistant to reduction are the lingual-mesial and buccal-mesial tubercles. Lingual-mesial tubercle bigger though buccal-mesial the tubercle is slightly higher than it. At the mesial and distal edges of the crown, the tubercles are connected marginal scallops, of which the mesial one is better developed. Buccal-distal And lingual-distal the tubercles are smaller and often subject to reduction (especially the lingual-distal one). The listed tubercles are separated from one another by grooves. Buccomesial groove goes at an angle and separates the buccal-mesial tubercle. The groove is divided into buccal and mesial parts. The latter can branch (rarely on the 1st molar). Branching of the buccal part of the groove can lead to the formation of a second ridge connecting the buccal mesial and lingual mesial cusps. Second furrow lingual-distal, separates the lingual-distal tubercle. This groove is arcuate, and there are distal and lingual parts. The buccal-mesial and lingual-distal grooves are connected in the center of the crown by an oblique groove, which is called fovea.
Lingual-distal tubercle usually well developed and can protrude in the lingual-distal direction, forming a well-shaped corner of the crown of the same name. Relatively rarely, the lingual-distal tubercle is subject to reduction up to almost complete disappearance (three-tubercle teeth). Buccal-distal tubercle usually well expressed, but may have signs of reduction. In such cases, it is smaller than the lingual-distal tubercle. On the surface of the buccal and lingual-mesial tubercles (the set of these 3 tubercles in odontology is called a trigon), and sometimes on the lingual-distal one, there are 3 ridges: median and 2 lateral - mesial and distal, which are separated by grooves. The ridges are directed mainly towards the central fossa. These ridges can form small additional tubercles on the cutting edges of the crown.
The mesial and distal contact surfaces of the 1st molar crown are larger than the buccal and lingual contact surfaces. A protrusion is quite often noticeable on the lingual surface - abnormal tubercle (tuberculum anomale).
The buccal and lingual contours of the crown are evenly convex, and the lingual contour has a greater curvature due to the mesial-lingual elevation. The slopes of the buccal-mesial and lingual-mesial cusps are clearly visible. The enamel-cementum border is straight or slightly arcuate. Interradicular leakage of enamel on the lateral surfaces is less common than on the cheek.
The lingual surface of the crown, like the buccal surface, is usually divided median sulcus into two halves. The groove on the first molars is well expressed and passes at the neck of the tooth into the root longitudinal groove of the lingual root. At the mesial surface, a mesial-lingual elevation is often noticeable, slightly not reaching the occlusal surface; its dimensions vary quite significantly. In fact, this elevation is the 5th occlusal cusp. It is separated by a transverse groove from the mesial-lingual tubercle.
The first upper molar has 3 root: buccal-mesial, buccal-distal and palatal. Buccal mesial root widest, flattened in the mesiodistal direction. Usually this root is longer than the buccal-distal one. The buccal contour of the buccomesial root is slightly convex, and the lingual contour is straight or slightly concave. There is often a longitudinal groove on the mesial surface of the root. From the distal surface of the tooth it is noticeable that buccal distal root the shortest, it is devoid of longitudinal grooves. Fusion of the buccal-distal root with the lingual root is possible. The palatal root is usually straight and sharply deviated lingually and distally, flattened in the buccolingual direction.
The crown cavity is wide and generally follows the shape of the crown. Cavity projections extend to the tops of all tubercles. The largest protrusion goes to the lingual-mesial tubercle. The bottom of the cavity is convex in the center, and in the corners it forms 3-4 funnel-shaped depressions, from which the root canals begin. The buccal mesial root often has 2 canals. Root canals vary in width. The lingual root canal is the widest, it is rounded and has a large volume. With age, the cavity of the tooth decreases.
The height of the crown on the buccal surface is 6.0-8.5 mm, the mesiodistal size of the base of the crown is 9-11 mm, buccolingual - from 11 to 13 mm; root length: lingual - 13.5-16.0 mm, buccal-distal - 10.0-13.5 mm, buccal-mesial - 12-14 mm.
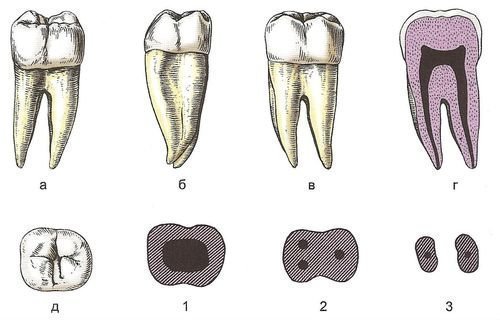
2nd upper molar may be very similar to the first molar, but may also differ from it (Fig. 2). The crown of the 2nd upper molar is compressed in the mesiodistal direction. Little visible on the buccal surface buccal-mesial, buccal-distal tubercles and median sulcus crowns, turning into an interradicular groove.
Rice. 2. Second upper molar, right:
a — vestibular surface; b — mesial surface; V - lingual surface; d — vestibulo-lingual section; d — mesiodistal section; e - cutting edge; 1, 2, 3 - shape of cross sections at the level of the crown, middle and upper third of the root, respectively
The occlusal surface has the greatest differences, which is associated with reduction processes lingual-distal And buccal-distal tubercles. In approximately half of the observations, 4 cusps are found on the occlusal surface of the 2nd upper molar, although the lingual-distal one is, as a rule, significantly smaller than that of the 1st molar. In 30-40% of cases, a tricuspid 2nd molar is found, in which the lingual-distal cusp is completely reduced on the occlusal surface, and lingual-mesial large and shifted in the lingual direction. Very rarely (in 5-10% of cases) the so-called compression form 2nd molar, which is a type of tricuspid molar. In such cases, all 3 cusps are located along a long diagonal running from the bucco-medial angle to the lingual-distal angle of the crown. Very rarely (up to 5%) the 2nd upper molar can be bicuspid. The origin of such a tooth is explained by the complete reduction of the buccal-distal and lingual-distal cusps and the strong development of the mesial ones. The double-cusped molar is similar to the upper premolars. Often on the occlusal surface the buccal part buccal mesial groove branches and forms along the bucco-mesial tubercle anterior to the occlusal fossa, the anterior fossa between the distal and median ridges of the bucco-distal tubercle. Near the central fossa, the posterior fossa is formed.
A feature of the relief of the contact surfaces is the displacement of the median groove on the distal surface of the crown due to the reduction of the lingual-distal tubercle in the distal direction.
A slight narrowing of the crown is determined on the lingual surface. When the lingual-distal tubercle is reduced, one protrusion formed by the lingual-mesial tubercle is revealed on the cutting edge of the lingual surface. The median groove of the crown in such cases moves distally (with a decrease in the lingual-distal tubercle) or is absent (with a complete reduction of the lingual-distal tubercle). Mesial-lingual crown elevation on the 2nd molar is rare.
Roots, usually 3 of them, when examining the tooth from the side of the contact surfaces, can have a divergent, parallel or converging direction. Sometimes palatal and buccal-mesial the roots grow together. In these cases, a longitudinal groove is visible along the line of fusion of the roots. Rarely there are 4 roots. Buccal distal root has the smallest dimensions. The palatal root is shorter than that of the 1st molar and deviated distally. The buccal roots are also deviated distally.
The crown cavity corresponds external form crowns With 3 tubercles, the cavity has 3 horns. Continuing into the roots, the cavity forms 3 channels. When the lingual and buccal-mesial roots fuse, there are 2 root canals in the fused root.
The height of the crown is 6-8 mm, the mesiodistal size of the base of the crown is 8-11 mm, the buccolingual size is from 10.5 to 13 mm; root length: lingual - 13.0-15.6 mm, mesial buccal - 11.0-13.6 mm, distal buccal - 9.7-13.0 mm.
3rd upper molar(wisdom tooth) is the most variable tooth in shape and size (Fig. 3). The crown of the tooth is the shortest. Most common form The occlusal surface is tricuspid with two buccal and one lingual cusps. With this form, the lingual-distal tubercle is reduced. The tricuspid 3rd molar often has compression form. Less commonly, there is a four-cusped form, similar to the shape of the 2nd molar. Rarely, a double-cusped molar is observed, in which the buccal-distal and lingual-distal cusps have undergone reduction, and the mesial cusps have shifted to the middle of the cutting edges of the crown. The size of the 3rd upper molar is reduced. Sometimes almost all of its tubercles are reduced. Only one tubercle remains, homologous buccal mesial tubercle. Such a tooth is called pin-shaped.
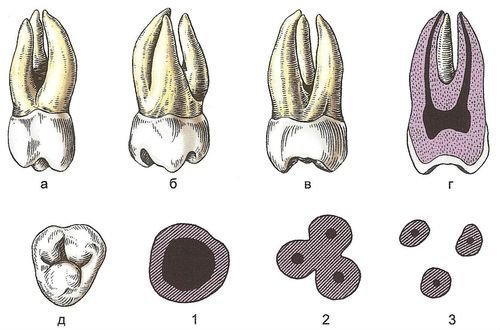
Rice. 3. Third upper molar, right:
In rare cases, the 3rd molar develops additional tubercles: on the distal surface - distomolar and on the vestibular surface - paramolar. Contact facet present on the 3rd molar only on the mesial surface. The 3rd molar can have 1-5 roots, more often there are 3 roots: palatal and two buccal.
The cavity of the tooth corresponds to its shape. In a four-tubercle tooth, the crown cavity has 4 horns, in a three-tubercle tooth - 3, in a two- and one-tubercle tooth - 2 and 1, respectively. There are usually 3 root canals; A single-rooted pin-shaped tooth has one root canal.
The height of the crown does not exceed 6 mm, width - 8-12 mm; root length: lingual (palatal) - 12.7-15.5 mm, medial buccal - 10.0-13.7 mm, distal buccal - 9.3-13.0 mm.
The upper molars are located in the dental arch almost under straight or slightly curved diverging lines, so the angles of inclination of the upper molars increase from the 1st to the 3rd. In the upper row of molars, the 1st is stable, the 2nd and especially the 3rd are variable. Hypodontia is often encountered, manifested in the absence of the 3rd molar. There are also frequent cases of retention (non-eruption), position anomalies, distal or buccal deviation. Less commonly observed is hyperdontia, in which the 4th molar is found, more or less formed or underdeveloped and fused to the 3rd molar with the formation of an additional distomolar tubercle.
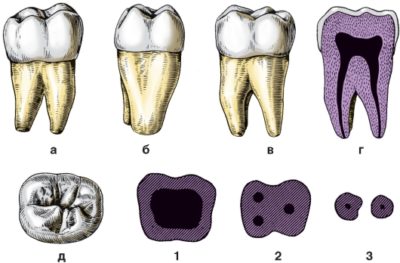
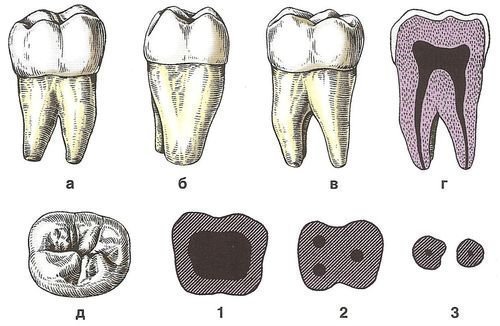
Lower molars (molars). The crowns of the lower molars are cubic in shape, on the occlusal surface there are usually 4 tubercles (from 3 to 6); teeth, as a rule, have 2 roots - mesial and distal, rarely - one root.
On the vestibular (buccal) surface there is a slight narrowing of the crown towards the root (Fig. 4). The surface of the crown is usually divided into 3 parts by two grooves. One of the grooves, which is a continuation of the buccal groove on the occlusal surface, is located closer to the mesial edge. Its depth and length vary. More often it is deeper near the cutting edge of the crown and, gradually flattening, reaches the lower third of the crown (less often, almost to the neck of the tooth). Rarely does this groove end in the middle third of the crown, where a rather deep vestibular fossa (fossa vestibularis), the meaning of which is unclear. Distal from the described groove there is a second groove, less deep and shorter. As a result, 3 elevations are formed on the buccal surface of the crown, especially pronounced near the cutting edge, where they end in tubercles, and disappearing towards the base of the crown. Rarely, on the buccal surface of the crown, an independent branch branches off from the mesial groove. arcuate groove, open to the base of the crown that surrounds additional tubercle. This tubercle can be barely noticeable or large, almost reaching the level of the occlusal surface and having its own horn in the cavity of the crown. The enamel-cement border on the buccal surface of the tooth can be convex towards the root, straight or concave and have enamel streaks.
Rice. 4. First lower molar, right:
a — vestibular surface; b — mesial surface; c - lingual surface; d — vestibular-lingual section; d — mesiodistal section; c - cutting edge; 1, 2, 3 - shape of cross sections at the level of the crown, middle and upper third of the root, respectively
On the occlusal surface, which is most often asymmetrical (pentagonal), there are 5 tubercles; 3 tubercles are located on its buccal half: buccal-mesial, buccal-distal And distal tubercles. They are separated by 2 grooves: the vestibular (between the buccal-mesial and buccal-distal tubercles) and vestibular-distal. There are 2 cusps on the lingual half of the occlusal surface of the crown: lingual-mesial And lingual-distal, separated lingual groove. In turn, both mesial tubercles are separated from one another mesial groove. The continuation of the mesial groove onto the distal half of the crown is called distal groove, which is divided into buccal-distal And lingual-distal, limiting the distal tubercle. All of the listed tubercles have the shape of a triangle, sometimes with a cut off apex (trapezoidal). Usually the buccal-distal and lingual-mesial cusps are in contact with their central departments. On the occlusal surface of the tubercles there are median, main and edge scallops oriented towards occlusal fossa. Their development and relief patterns are different, which has implications for anthropologists.
Rarely, the lingual groove branches and separates from the lingual-mesial or lingual-distal tubercle a section on which an additional internal middle tubercle(lingual-medium). In such cases, the occlusal surface takes on a six-tubercle shape. Very rarely, an additional 6th cusp may form between the lingual-distal and distal cusps as a result of branching of the lingual-distal sulcus. This tubercle on the 1st molar is less common than on other lower molars.
When examining the proximal (contact) surfaces, the inclination of the contour of the buccal surface of the crown in the lingual direction is noticeable. The contours of both the buccal and lingual surfaces of the crown are slightly convex and arched. On the mesial and distal surfaces of the crown, close to top edge, short shallow grooves are noticeable, and on the mesial surface the groove is shifted in the lingual direction. Along the edges of the buccal and lingual surfaces there are wide ridges originating from the tubercles. Contact facet on the mesial surface it is located on the bucco-mesial tubercle, and on the distal surface it is on the bucco-distal tubercle. Enamel-cementum junction at contact surfaces runs along a straight or slightly convex line with a slope towards the buccal surface. Enamel leaks are rare.
The lingual surface is divided longitudinal groove into two approximately equal halves. The central ribs of the tubercles converge at an obtuse or (rarely) right angle.
In the vestibular norm, two roots are visible - mesial and distal. Mesial root wide, wedge-shaped, with pronounced ridges along the edges, between which there is a wide depression. The apex is deviated vestibularly. Distal root narrower and shorter than mesial. Usually its surface is flat or evenly convex. Sometimes the distal root is split into two: buccal and lingual, of which the latter is usually thinner and shorter. More often, both roots diverge, less often they form a barrel-shaped figure (in the initial part they diverge, and in the lower half they converge), run parallel or converge. The apices of both roots are usually deviated distally. Both roots are strongly flattened in the mesiodistal direction. The roots of the 1st lower molar do not fuse.
The cavity of the crown is cuboidal, with 5 or 6 horns in the direction of the occlusal cusps. The largest volume has buccal-mesial horn, both cheek horns are the highest. Mesial root, as a rule, has 2 channels. In the distal root, 2 canals are found in half of the cases.
The height of the crown of the 1st lower molar is 6-8 mm, the mesio-distal size of the crown is 10-13 mm, the buccolingual size is 9-12 mm; the length of the mesial root is 14-16 mm, the distal one is 13.4-14.6 mm.
The 2nd lower molar has a cubic crown (Fig. 5). On the buccal surface of the crown there is a pronounced vertical furrow, dividing the crown into two convex halves. Additional tubercle is rare. The enamel-cementum boundary is almost straight.
Rice. 5. Second lower molar, right:
a — vestibular surface; b — mesial surface; c - lingual surface; d — vestibular-lingual section; d — mesiodistal section; e - cutting edge; 1, 2, 3 - shape of cross sections at the level of the crown, middle and upper third of the root, respectively
The occlusal surface is almost square and often bears 4 tubercles: 2 buccal (mesial and distal) and 2 lingual (mesial and distal), separated from one another by 4 grooves, which are called the mesial, buccal, distal and lingual surfaces, respectively. They all converge and form the occlusal fossa. Less commonly, there are 5 tubercles with additional formation distal tubercle. On the occlusal surface of the 2nd lower molar there are very rarely 6 cusps, and as a result of the formation of an additional buccal-median cusp.
Found on the lingual surface inferior medial lingual eminence. It is located below the lingual-mesial tubercle, sometimes reaching large sizes; it may have an additional root.
A tooth usually has two roots - mesial and distal. They are located almost parallel, their apices are deflected distally. The roots can grow together completely or only on the buccal surface, being isolated on the lingual.
The cavity of the crown is cubic in shape, with 4 horns in the direction of the masticatory tubercles. There are two canals in the mesial root, usually one in the distal root, and very rarely two.
Crown height - 6.0-8.5 mm, mesiodistal size - 9-12 mm, buccolingual - from 8 to 11 mm; root length: mesial - 11.0-14.5 mm, distal - 9.5-14.0 mm.
The 3rd lower molar is also called a wisdom tooth (Fig. 6). It is variable in shape and size. This tooth is smaller than other lower molars, but larger than upper tooth wisdom, especially in the mesiodistal direction. On the occlusal surface of the crown, in 50% of cases there are 4 cusps, in 40% - 5, in 10% of cases - 3 (one of the distal cusps is reduced) or 6 (the 6th cusp lies between the lingual-distal and distal cusps). There is strong folding of the crown. On the distal part of the lingual surface of the 3rd lower molar, it occurs more often than on others. inferior mesial-lingual eminence.
Rice. 6. Third lower molar, right:
a — vestibular surface; b — mesial surface; c - lingual surface; d — vestibular-lingual section; d — mesiodistal section; c - cutting edge; 1, 2, 3 - shape of cross sections at the level of the crown, middle and upper third of the root, respectively
A tooth has two roots, less often - one. The roots are short, deviated distally, and sometimes grow together.
Crown cavity irregular shape, has horns according to the number and position of the chewing tubercles. With two roots, there are two root canals in the mesial one, and, as a rule, one in the distal one (Fig. 7).
Rice. 7.
The height of the crown does not exceed 5.5 mm, the mesiodistal size is 6-11 mm, the buccolingual size is from 6 to 9 mm; root length: mesial - 11.0-14.5 mm, distal - 9.5-14.0 mm.
In the dental arch, the lower molars lie almost in a straight line. Stable, as in the upper dentition, is the 1st lower molar, the most variable is the 3rd. Various possible position anomalies molars, especially the 3rd (rotations, displacements from row to side, etc.). Happens congenital absence 3rd molar, as well as its retention. There may be a 4th molar, more often on the lower dental arch than on the upper. The vertical axes of the crowns of the lower molars have an inclination in the opposite direction relative to the inclination of the upper molars. When the jaws are closed, the row of upper molars normally overlaps the row of lower molars with a slight shift upper teeth in the distal direction. As a result, each tooth comes into contact with two teeth: the corresponding one and the next one.
Human anatomy S.S. Mikhailov, A.V. Chukbar, A.G. Tsybulkin
U healthy person 28 or 32 teeth grow in the oral cavity. It all depends on whether you already have wisdom teeth or not. But not all people know the answer to the questions of what the correct name is for each tooth and what molars are. However, everyone should have at least a small understanding of the structure of the oral cavity and the location of the teeth.
Molars are the fourth and fifth teeth in the order of eruption in the primary row or from the sixth to eighth row of permanent teeth on the right and left sides of the jaw. They are located behind the premolars. Very rarely, so-called additional, fourth.
Typically, molars have four canals and three roots in the upper jaw, and three canals and two roots in the lower jaw. Upper first molars may have three canals in 7%, four canals in 90%, and five canals in only 3% of cases. In 40% of cases, the upper second teeth may have four canals. Upper third molars may have two, four, or five roots.
The roots of the molars extend from the cavity of the tooth in the form of thin branches. On the line that connects the mouth of the palatal canal and the mouth of the mesiobuccal canal, the mouths of the fourth upper first and second molars are also located.
On the lower jaw, the first molar is in size more than the second and third.
On the human lower jaw, the first molar has five cusps on the chewing surface - two oral and three vestibular (distal, medial vestibular). The second one has four tubercles - two oral and two vestibular (distal, medial vestibular).
![]() When baby molars fall out, it is not the molars that erupt, but the premolars. Many parents cannot understand the reason for this order of teething. This is explained by the fact that in all children the oral cavity increases in size, and the molars erupt behind the primary molars. Premolars have smaller size
, rather than the indigenous ones, and they are located behind the fangs. The first premolar has two roots, all the others have one. There are eight premolars in the human oral cavity (four premolars on each jaw).
When baby molars fall out, it is not the molars that erupt, but the premolars. Many parents cannot understand the reason for this order of teething. This is explained by the fact that in all children the oral cavity increases in size, and the molars erupt behind the primary molars. Premolars have smaller size
, rather than the indigenous ones, and they are located behind the fangs. The first premolar has two roots, all the others have one. There are eight premolars in the human oral cavity (four premolars on each jaw).
In the primary dentition there are no premolars, unlike molars. After all, small child The jaw has not yet grown to a size that can accommodate so many teeth. Despite the fact that premolars are considered the smallest molars, they are not very small in size. Premolars also perform functions of chewing and grinding food. In their shape they are similar to fangs, only their crown is much wider than that of fangs. There are only two cusps on the crown of the premolar.
The appearance of baby teeth molars
Surely every parent remembers that period in the life of their baby when his molars began to erupt. After all, cutting through them is more painful than others. The only exception in this case are fangs. Molars erupt earlier than canines, although in their location they are behind them.
The first molars begin to appear when the child is already reached 12 one month old . They erupt like all others - in pairs. The molar appears first on the lower jaw, then on the upper jaw. Ideally the first molars milk type should appear before the baby is 18-20 months old. During this same period of a child’s life, the most painful teeth, the fangs, may begin to come out. That is why age up to 24 months is considered the most active age eruption of painful teeth.
Now, as for the second molars of the deciduous type, they appear at the age of 2 years. Sometimes they can erupt either earlier or a little later. But when the child is 30 months old, he should already have both first and second molars. Don't worry if your baby has any deviations from the due dates. This may not always be a pathology. This may also be due to genetics and heredity.
Replacement of primary molars with permanent permanent molars
 Children begin to replace teeth from about five years of age. Moreover, this replacement begins precisely with the molars. Replacement has the opposite order of appearance. Molars appear in the free space that appears due to jaw growth. Therefore, they do not replace any teeth. Precisely because they do not replace - they are the last and permanent teeth located behind the baby molars. Sometimes the first molars can also be called six-year-old molars. After all, it is at this age that they begin to exist.
Children begin to replace teeth from about five years of age. Moreover, this replacement begins precisely with the molars. Replacement has the opposite order of appearance. Molars appear in the free space that appears due to jaw growth. Therefore, they do not replace any teeth. Precisely because they do not replace - they are the last and permanent teeth located behind the baby molars. Sometimes the first molars can also be called six-year-old molars. After all, it is at this age that they begin to exist.
At the age of 9-12 years, primary molars fall out. They are replaced by molar premolars. They appear at about 10-12 years of age, almost immediately after the dairy ones that fell out. By the age of 14, the average person does not have a single milk jug. In the practice of dentistry, there were some exceptions when milk jugs did not fall out until 18 (and sometimes longer) years.
If you experience early loss (before 5 years), you should consult a doctor. This could be the reason malocclusion, trauma, advanced caries or deliberate loosening.
Is it possible to loosen baby molars?
A molar tooth that appears after a year is a milk tooth. So one day it will start to wobble and fall out. To make it fall out faster, many parents, upon learning that their child’s tooth is loose, suggest loosening it themselves. At the same time, parents do not think about whether this can be done and whether this will entail any consequences in the future. Everyone in childhood is taught that if a tooth is loose, then it needs to be helped to fall out.
But experts have a completely different opinion on this matter. They claim that doing this is strictly prohibited. They say that by accelerating the natural process of hair loss jaw growth may slow down. And what follows is that the appearance of the radical constant will not be in the place intended for it. Very often the cause of crooked teeth in adulthood is wrong actions when changing them.
This also applies to molars. milky looking. You cannot loosen them to speed up the process of falling out. Do not disturb the order of natural preparation maxillofacial apparatus baby for teeth replacement.
Signs of imminent appearance of molars
The signs of the imminent appearance of molars are slightly different from the signs of primary molars.
When milk appears:

When molars emerge, the following is observed:
- jaw enlargement;
- appearance free space behind milk molars;
- the appearance of gaps among the teeth - trems;
- loosening of baby teeth.
Exactly where it was formed free space and the root one will soon erupt. Trems are needed for the even placement of molars in the oral cavity. When present, crowding and curvature are avoided. Also, their absence can cause malocclusion. If this happens, the child may have to wear lingual braces or braces.
Helping your child replace teeth
Very often, parents think that when changing baby teeth to molars, the child experiences mass painful sensations . But in reality this is not the case. If you do not help this process, the milk roots will gradually dissolve and the milk roots will fall out on their own. Or if it seems to you that the tooth is hanging at the very tip. then you can pull it slightly and get it out.
You need to be able to explain to your child during the period of milk rupture that he needs to rinse his mouth for disinfection purposes. Rinse oral cavity you can use regular warm water, chamomile decoction or special means, which is sold at the pharmacy.
There are also cases that after a tooth falls out, the hole in which the tooth was located may bleed for some time. In such situations, apply a cotton swab to your baby and ask your baby to bite it with his teeth. If the hole is bleeding, then it is undesirable to eat or drink for at least two hours after the prolapse.
If tooth replacement occurs with swelling of the gums, increased body temperature and strong painful sensations You should consult a doctor immediately. The normal change from dairy to indigenous occurs with virtually no symptoms.
Molars and prevention of their loss
When your child already has all his molars “assembled,” it is necessary to proper care behind them. If a molar is lost, a new one will not grow to replace it. Therefore, a responsible step falls on parents. This step is to teach your child how to properly care for his or her mouth.
Proper hygiene includes:
It is also better for the child to know that he needs to give up drinks with gases and eat sweets in smaller quantities. After all, when consuming such products, it may occur destruction of tooth enamel.
You need to use foods rich in vitamins and calcium in your diet. Calcium is essential for healthy gums and teeth. And if your child has healthy gums, then his teeth will be healthy.
Children have 8 molars in the jaw, and in adolescents and adults their number ranges from 8 to 12. Their number in the permanent dentition depends on how many eights have erupted in the person. Large molars of the upper jaw usually have 3 roots, and lower molars have 2. The number of canals may vary; it happens that there are several canals in one root. It is in the roots of this group that difficult and curved canals are most often found.
What do they look like?
Molars are the teeth with the largest crown. The shape of their crowns on the upper jaw is similar to a rhombus, and the crowns on the lower jaw are cubic in shape. As a rule, on their chewing surface there are 4 or 5 tubercles, and sometimes 6. The tubercles are called buccal and lingual, depending on their location - closer to the tongue or to the cheek. The distant tubercles are called distal, the near ones are called mesial. The tubercles are separated by grooves called fissures. Eights are not always the case. Sometimes they remain impacted, that is, located inside the jaw. The shape of their crowns can be very different.
When can I expect my baby to get big molars?
When a child turns one year old, you can expect that the first molars will very soon appear on the upper jaw on the left and right. And after 1 - 2 months - the first molars on the lower jaw. The second lower molars appear earlier than the upper ones - at approximately 1 year 8 months. And the upper second ones erupt at 2 - 2.5 years.
Differences between primary and permanent teeth
--noindex-->When a child has both primary and permanent molars in his mouth, the primary teeth can be recognized by the following features:
- temporary ones are smaller in size than permanent ones;
- in milk teeth you can observe a bluish-white tint of the enamel, while permanent teeth are more likely white-yellowish;
- the roots of primary molars are shorter and wider;
- in the primary occlusion, abrasion of the tubercles can be observed on the chewing surface. This phenomenon is called “physiological abrasion”;
- in temporary dentition it often develops on the lateral surface, and in permanent teeth in childhood The chewing surface is usually affected;
- Normally, primary molars fall out and are replaced by permanent ones. When the time comes to change the bite, the molar begins to wobble.
Timing of eruption of permanent molars
So, the child has his first permanent molars, the sixth teeth erupt starting at the age of 6 - 7 years. The bottom six appears first, and then the top one. Sevens appear in adolescence usually at 12 years of age. And wisdom teeth can grow at the age of 17, or much later. Dentists often observe x-ray the patient lacks the rudiments of eights.
How do dentists treat distant teeth in adults and children?
--noindex-->Some treatment features:
- Often in the area of fissures of molars, they are done to prevent the development of caries. This procedure is relevant in childhood and adolescence, when the mineralization of the enamel has not yet been completed.
- During treatment deep caries lower molars are often found. This is due to the fact that medial horn they are located quite high and microorganisms from deep carious cavity begin to destroy pulp tissue. Sometimes such pulpitis can be cured biological method, that is, there is no need to perform pulp removal.
- When depulpation is performed (the pulp is removed and the canals are cleaned), the patient needs to be prepared for the fact that he will have to sit in the dentist’s chair for a long time. The fact is that it takes a lot of time to go through and thoroughly clean the channels. In pediatric dentistry, treatment of molar pulpitis occurs faster; the child’s teeth are treated without the use of files to pass through canals. After all, when passing through the children's canal with a sharp file, damage to the rudiment located inside the jaw is possible.
- Very often the number eight has to be removed. If it is impacted, an incision is made into the mucosa, then the doctor makes a small hole in bone tissue and through it pulls out the crown and roots.
Even though molars are located at the far end of the mouth, they also contribute to the beauty of a smile. Often it is because of them that malocclusions develop. And the loss of a molar, especially at a young age, is completely undesirable. Therefore, you should try to preserve your own large molars for as long as possible!
Chewing teeth or molars are separate species, which requires special consideration. Every person has them, and they include. Although they total quantity not much. You can even check it in your own mouth if you count the largest formations.
What are molar teeth?
Molars- these are the most large teeth responsible for chewing food. This is their main function, not performed by the rest of the jaw. Because of this, the rules of oral care clearly indicate mandatory daily brushing to remove all food debris. You will have to take care of this to prevent early loss.
The total number of molars reaches 12, but only if all 4 wisdom teeth grow. The latter cannot grow until the age of 6, so babies have to chew with only 8 molars. Although this does not bother them at all and does not affect their daily nutrition.
Unique structure
 Molar teeth have a unique structure. They become the basis of all chewing movements made by a person. Moreover, there is big difference between different entities, therefore it is necessary to highlight several important features:
Molar teeth have a unique structure. They become the basis of all chewing movements made by a person. Moreover, there is big difference between different entities, therefore it is necessary to highlight several important features:
- The first tooth is larger in size than the others.
- The root of the first tooth is much stronger than the subsequent ones.
- On the lower jaw the tooth has a triple root.
- On the upper jaw the tooth has a double root.
- There are 3 to 5 cusps on the crown of the molars.
- On the crown of the upper molars the cusps are much sharper.
The structure is varied, which complicates treatment. Only in large dental clinics do doctors undertake complex procedures and operations. In ordinary hospitals, specialists rarely take on such problems, due to a lack of tools and equipment. Accordingly, when pain appears, you need to turn to professionals, and not try to cope with it with folk remedies.
Difference between molars and premolars
 Parents often confuse molars and premolars in their children. When, after the first milk teeth fall out, new ones come out right next to the fangs, they should not be confused. These are not molars, but premolars. They are also chewable, but are significantly smaller in size.
Parents often confuse molars and premolars in their children. When, after the first milk teeth fall out, new ones come out right next to the fangs, they should not be confused. These are not molars, but premolars. They are also chewable, but are significantly smaller in size.
Premolars appear quickly, but they are not dairy. Moreover, during their growth, they often have to drink, since the neighborhood turns out to be critical. Parents should pay special attention to this point, because simultaneous development entails serious consequences, because of which adults must monitor the process.
When do the first primary molars appear?
 First teeth Primary molars appear at approximately 2 years and 5 months. At this time, the chewing reflex is fully developed, so the child immediately begins to use them. Without them, food consumption remains problematic, but doctors still recommend giving hard foods to speed up the process of jaw development.
First teeth Primary molars appear at approximately 2 years and 5 months. At this time, the chewing reflex is fully developed, so the child immediately begins to use them. Without them, food consumption remains problematic, but doctors still recommend giving hard foods to speed up the process of jaw development.
At this age, parents often consider their children adults. The canines grow the most painfully, but even molars can create a lot of problems. Sharp tubercles on their crown sharply break through the surface of the gums, so the baby has to suffer. During this period, special painkillers should be given that will not harm the body. Their list is clarified by the dentist or pharmacist at the pharmacy. Using this information, you will be able to purchase the appropriate syrup for babies.
When do primary molars become molars?
 Growing teeth – complex process, and replacing dairy with indigenous ones creates the most trouble. Because of this, parents need to know for sure that molars change between 11 and 13 years of age. They become the last in the rows on the jaw, but this does not affect their condition. Without care, crowns deteriorate much faster than incisors or canines, so even in adolescence you have to deal with troubles.
Growing teeth – complex process, and replacing dairy with indigenous ones creates the most trouble. Because of this, parents need to know for sure that molars change between 11 and 13 years of age. They become the last in the rows on the jaw, but this does not affect their condition. Without care, crowns deteriorate much faster than incisors or canines, so even in adolescence you have to deal with troubles.
The replacement of primary molars with permanent molars occurs in a complex manner. New ones grow right under the old ones, so the loss occurs irregularly. In some cases, replacement does not even occur, so that milk formations remain right up to the first wisdom teeth. This should not bother a person, but it is still better to visit a dental clinic to make sure there is no malocclusion or jaw development.
Will loosening help speed up growth?
![]() When forming the jaw, some parents try to speed up the process. When they notice loosening, they support it, hoping that a new molar will appear immediately after it falls out. Dentists try to predict such a mistake, arguing that it is impossible to do this. The consequences of such actions become the most problematic. What are the doctors talking about?
When forming the jaw, some parents try to speed up the process. When they notice loosening, they support it, hoping that a new molar will appear immediately after it falls out. Dentists try to predict such a mistake, arguing that it is impossible to do this. The consequences of such actions become the most problematic. What are the doctors talking about?
- Incorrect positioning of molars;
- Malocclusion;
- Improper jaw growth.
Wrong actions lead to dire consequences. The natural process cannot be disrupted in any way, so it is better to wait until the tooth gradually loosens on its own and falls out. In this case, there will be no negative effects, and the condition of the jaw will remain ideal.
Parents need to come to dental clinics regularly. Crooked teeth most often appear during the process of changing baby teeth to molars, after which it is necessary to install braces. They will help correct the bite, but for the child the procedure usually entails stress. So there is no need to allow unpleasant consequences.
How to notice the eruption of molars?
 Molars– teeth whose growth is difficult to notice. In childhood, the baby faces terrible symptoms, and later practically does not notice what is happening. When a new formation appears in the near future, trems immediately become visible. These are small gaps that will be filled with a new part of the jaw.
Molars– teeth whose growth is difficult to notice. In childhood, the baby faces terrible symptoms, and later practically does not notice what is happening. When a new formation appears in the near future, trems immediately become visible. These are small gaps that will be filled with a new part of the jaw.
Only in infancy Parents have to deal with pain in their children. Later this process is not attractive special attention, passing almost unnoticed. The only problem is minor discomfort associated with jaw enlargement.
Important! If your child suddenly develops a fever, you should immediately consult a doctor. In this case, it is a sign of a developing inflammatory process.
Helping your child change teeth
 Changing baby teeth for molars is safe, but there are certain tips for parents. They need to be taken into account in order to eliminate even minor troubles. Children are not aware of what is happening, so they need some help.
Changing baby teeth for molars is safe, but there are certain tips for parents. They need to be taken into account in order to eliminate even minor troubles. Children are not aware of what is happening, so they need some help.
- When a tooth falls out, you need to wait until the last moment and just pick it up.
- After falling out, a small wound remains on the gum where dirt can get in, so it is better to teach your child to rinse the mouth.
- If the wound is bleeding, you can use soda solution and postpone eating for 2-3 hours.
A visit to the dental clinic is usually not required. In rare cases, a tumor may appear or begin, and a specialist examination will be needed. If parents take the process seriously, dangerous consequences will not happen, so the child will not have to deal with the unpleasant procedure once again.
Preservation of molars
 Parents are obliged to early age teach children to take care of the oral cavity. Some people prefer, but first of all you need to follow simple rules. What should I do?
Parents are obliged to early age teach children to take care of the oral cavity. Some people prefer, but first of all you need to follow simple rules. What should I do?
- Be sure to brush your teeth 2 times a day.
- Toothpaste should contain calcium and fluoride.
- During the day, it is worth rinsing your mouth several times to remove food debris.
- Parents should reduce the amount of soda and sweets for children.
- Instead of complex vitamins, it is better to enrich your diet with calcium.
Parents should explain to children that molars will remain forever. New ones will not grow in their place; you should take care of them, eliminating the risk of damage to the enamel and roots. Yes, there are causes of destruction that are independent of humans, but cases of their occurrence are rare.
Molars or chewing teeth- a small part of the jaw that performs the most important function grinding food. Their number is small, but even these formations require regular inspection dental clinic And daily care. This point remains the most important, so you should not forget about it in order to keep your own smile in perfect shape.
Educational video: molars, dental anatomy
We recommend reading
 Degas E. “Blue Dancers. Essay based on the painting by Edgar Degas “Blue Dancers Dancers in Blue”
Degas E. “Blue Dancers. Essay based on the painting by Edgar Degas “Blue Dancers Dancers in Blue” We reflect in the RSV reimbursement of social insurance expenses for the last year Appendix 2 line 090 of the calculation of insurance premiums
We reflect in the RSV reimbursement of social insurance expenses for the last year Appendix 2 line 090 of the calculation of insurance premiums Olesya Malibu: Russian clone of Pamela Anderson
Olesya Malibu: Russian clone of Pamela Anderson The problem of human spirituality
The problem of human spirituality

