Classes dental caries By Black:I Class– cavities in the area of fissures and natural depressions. II Class– cavities on the contact surfaces of molars and premolars. The American scientist Black proposed a classification carious cavities by localization: 1 option It has been noted in the literature following changes: macroglossia, protos tongue, broken tongue, papillary hypertrophy, oval palate, craniofacial morphological changes, occipital bone and flattened nasal bone, dentofacial deficiency, caries lesions and buccal candidiasis. Typically, there are cases of periodontal disease and a low prevalence of caries in these patients. Their life expectancy has increased due to improved medical care. Recognizing the common oral characteristics of this syndrome can help the dental surgeon maintain the oral health of these patients by performing activities specific to the identified characteristics. Classes of dental caries according to Black: Down syndrome, also known as trisomy 21, is genetic disease, in which affected individuals carry an extra 21 chromosome. Patients with Down syndrome are considered special patients in dentistry and require differentiated care. Mental deficiency is one of the most modern characteristics in the development of a child with Down syndrome, which is likely to be justified by a global developmental delay, from child to child, developmental delays may occur due to mental deficits in the child. speech. Option 2 Classification of caries according to the location of the carious cavity (according to Black): Class I - caries in the area of fissures (natural grooves); Class II - caries of the contact surfaces of large and small molars; Class III - caries of the contact surfaces of the incisors and canines while maintaining the cutting edges; Class IV - caries of the contact surfaces of incisors and canines in case of violation of the cutting edges; The literature regarding oral conditions in patients with Down syndrome is extensive and sometimes contradictory. This study contributes important function constant review of research to have a critical diagnosis, facilitating decision-making in dental clinic when visiting and monitoring these patients. Due to the variability of the affected structures, the patient with Down syndrome requires specialized and multidisciplinary treatment. Clinical recognition of oral changes from the syndrome and early intervention by the dental surgeon allows for better prediction of the evolution and consequences of malformations, as well as improved living conditions. Class V - cervical caries.Classification by localization
Class I – cavities in the area of fissures and natural depressions.
Class II - cavities on the contact surfaces of molars and premolars.
Class III - cavities on the contact surfaces of the incisors and canines without breaking the cutting edge.
Class IV - cavities on the contact surfaces of the incisors and canines with a violation of the cutting edge and crown angles.
Class V – cavities on the labial, buccal, lingual surfaces located in the gingival part of the tooth crown.
Class VI - cavities located on the tops of the cusps of molars and premolars, as well as on the cutting edges of the incisors and canines.
Option 3 Treatment of caries according to Black
The purpose of this study was to identify oral characteristics of patients with Down syndrome in the current literature. The literature search was conducted in English, Portuguese and Spanish with the following descriptors: Down syndrome, Down syndrome, oral manifestations, oral manifestations, oral manifestations, malocclusion, malocclusion.
The inclusion criteria were articles describing clinical manifestations Down syndrome and in human populations of any age. Exclusion criteria were genetic, ultrastructural and animal studies or studies that were not related to Down syndrome.
Dental caries is pathological process progressive subsurface demineralization of enamel with the future formation of a cavity defect that occurs after teething under the influence of acids produced by microorganisms found in dental plaque.
Dental caries is considered one of the most common diseases of humanity. In many countries, the prevalence of caries is 95-98%. The incidence of dental caries worldwide is trending upward, especially among children.
For this study, 16 publications were selected based on inclusion and exclusion criteria. Down syndrome is one of the most common genetic changes. The literature regarding the oral conditions of patients with Down syndrome is extensive and covers two aspects: morphological aspects and the prevalence of oral diseases.
Craniofacial anomalies presented: macroglossia, protos tongue, fissured tongue, papillary hypertrophy, oval palate, flattening occipital bone and facial and nasal profile, dentoalveolar occlusion, tooth stains, carious lesions and buccal candidiasis.
Causes of caries
More than 400 theories have been proposed to explain the causes of caries, but the following are generally accepted:
For the development of caries it is necessary various conditions, in the presence of which there is a predisposition to this disease increases.
Risk factors
The teeth of these patients represent complete mineralization and, although retaining certain similarities in sequence and symmetry, they present variations in the eruption pattern. The prevalence of periodontal disease is high, especially in adults, and low frequency caries in patients with Down syndrome.
Macroglossia, which is congenital, is caused by excessive muscle growth. This is directly related to the patient's condition being gums, which can cause tooth dislocation and malocclusion, leading to protrusion and buccal opening as compensatory mechanisms.
General factors:
- Cariogenic diet with a predominance of carbohydrate foods (cookies, sweets, carbonated drinks).
- Changes in the patient's physical health ( frequent illnesses general respiratory diseases, FLU, etc.).
- Extreme stress on the body (radioactive radiation).
- Unfavorable heredity.
Local factors:
Another common defect is a cracked tongue. It is characterized as grooves on the dorsal surface that radiate from the central sulcus of the tongue. They are usually painless, however, they present painful symptoms when the accumulation of food waste causes irritation.
Children with Down syndrome present with a delay in tooth eruption, both in the primary and permanent dentition, compared to children without Down syndrome. The study analyzed 49 panoramic radiographs of people with the syndrome aged 3 to 33 years. Radiological characteristics of dental abnormalities were observed in both deciduous and permanent teeth in accordance with International classification diseases.
- Poor hygiene oral cavity(presence of soft plaque and mineralized dental deposits).
- Violation of the qualitative and quantitative composition of saliva (high viscosity, lack of calcium ions).
- Violation of the resistance of mineralized tooth tissues (due to surface changes in structure).
- Changes in biochemical composition enamel, dentin and cement.
- Pathological changes in the pulp apparatus of the tooth.
- Disturbances in the formation of the dental system
Development of caries and its symptoms
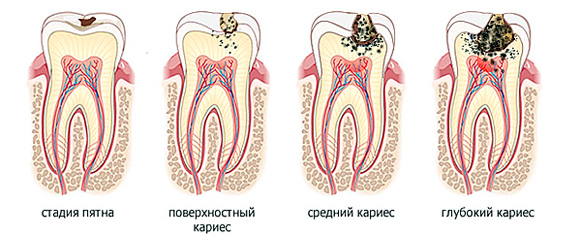
The development of caries occurs in several stages:
The authors found a high incidence of dental abnormalities in patients with this syndrome, as well as the presence of more than one type of abnormality in the same person. Among them: taurodontism, proven anodontia, suspected anodontia and conical teeth.
Treatment of caries according to Dr. Black's classes
Considering oral diseases, the literature is rich in aspects related to periodontal disease, susceptibility and prevalence of caries diseases, salivary flow, salivary pH and buffering capacity, and susceptibility to the development of oral candidiasis.
- Caries in the spot stage (initial caries). It is asymptomatic, the affected area of the tooth loses its shine, becomes dull, and a chalky stain forms. The spot may be pigmented (have yellowish color). Probing is painless.
- Superficial caries. Asymptomatic, sometimes painful sensations from sweet, sour, salty, less often from mechanical irritants. A rough defect up to 1 mm deep is detected on the tooth; the color of the defect may change to light brown. Probing is painless.
- Average caries. Complaints about short-term sharp pain from food getting into the tooth, from cold and hot, the pain goes away immediately after the irritant stops. A carious cavity in a tooth of small or medium size, up to 1.5-2 mm deep. Probing is painful along the dentinal-enamel junction.
- Deep caries. Complaints about painful sensations from all types of irritants, from cold, hot, from food getting into the carious cavity. A deep carious cavity filled with softened, necrotic dentin and food debris. Probing along the dentinal-enamel border and the bottom of the carious cavity is painful, there is no communication with the dental pulp.
In the case of periodontal disease in Down syndrome, the prevalence is between 30% and 40%, and in individuals close to the age of thirty, this percentage increases to approximately 100%. Older patients experience severe loss of alveolar bone, tooth mobility, and supra and subgingival calculus. It has been proven that periodontal disease is caused by local etiological factors, especially bacterial plaques, but some types of diseases and systemic disorders can reduce or alter host resistance or response and then predispose to periodontal changes.
Features of caries classification according to Black
In 1891 A. Black, based on patterns of distribution and typical localization, systematized all cavities, dividing them into 6 classes. The proposed classification is convenient for choosing tooth treatment tactics depending on the location of the defect. The purpose of this classification is to standardize methods of filling and preparing various carious cavities.
The real changes in patients with Down syndrome that increase the chances of developing periodontal disease are: poor oral hygiene, which determines the severity of the lesion, gums with poor healing potential, dietary factors, abnormal anomalies, interference with tooth eruption, morphology of altered teeth and malocclusion. There are also some authors who have concluded that the increased susceptibility to periodontal disease in these patients is associated with decreased resistance to bacterial infections and a higher prevalence of infection in periodontal tissues.
Classification of caries according to Black:

- 1st class– carious cavities located in the area of fissures and natural depressions of the chewing group of teeth and in the area of the blind fossa of the lateral incisor.
- 2nd grade– cavities on the mesial and distal surfaces of premolars and molars, limited by tooth tissue on three sides.
- 3rd grade– cavities on the medial and distal surfaces anterior group of teeth with no destruction of the cutting edge.
- 4th grade- cavities on the medial and distal surfaces of the anterior group of teeth with a violation of the cutting edge.
- 5th grade– cavities in the neck area of all groups of teeth.
- 6th grade– cavities on immune zones (tubercles of teeth, enamel ridges)
Treatment of caries
To reduce the risk of caries development, its prevention and treatment is required.
It is known that individuals with Down syndrome present changes in the immune system, which results in decreased chemotaxis and phagocytosis performed by neutrophils and monocytes. This neutrophil-deficient chemotaxis was correlated with increased alveolar bone loss together with the reduced number of mature T lymphocytes that are present in these individuals. Such characteristics may contribute to the progression of periodontal disease in patients with Down syndrome compared with normal individuals.
This fact is likely related to the increased salivary capacity of saliva and the tendency of these individuals to exhibit bruxism habits. In this case, the occlusal surfaces susceptible to caries are often smooth and worn by grinding teeth. Some authors also report that the low prevalence of caries in these people may be due to delayed tooth eruption and a large number diastema, which will significantly reduce the prevalence of proximal caries lesions.
Standard treatment includes:

- Examination, questioning, diagnosis, drawing up a treatment plan.
- Anesthesia.
- Opening a carious cavity (removing overhanging edges of enamel that do not have a dentin base).
- Expanding the cavity (improving visibility).
- Necrectomy (removal of softened dentin).
- Formation of a cavity (creation necessary conditions for filling).
- Finishing the edges of the enamel (creating a better fit of the filling to the tooth).
- Sealing (using composite materials and cements).
Filling teeth restores their 5 main functions: speech, chewing, aesthetics, maintaining the soft tissues of the face, creating an occlusal plane.
On the other hand, there are studies that discuss the connection between tooth decay and Down syndrome. Some local determinants of caries disease, such as poor oral hygiene and cariogenic diet, often overlap with “protective factors”; which will lead to a higher prevalence of dental caries in individuals with Down syndrome.
These factors can be added to high frequency with which these patients use sweetened medications indicated for sinusitis, otitis media, tonsillitis and others respiratory infections, common to this population. The authors conducted a comparative cross-sectional study with a sample of 15 individuals of both sexes and different ages. Seven people were hospitalized at PTA younger age, Down syndrome.
Methods for treating hard dental tissues:

- Mechanical- using rotary burs and hand tools).
- Chemical-mechanical- usage chemicals to soften non-viable tooth tissues with their subsequent removal.
- Pneumokinetic— the impact of directed supply of an abrasive substance in the form of an aerosol under pressure.
- Acoustic- ultrasonic.
- Laser preparation. Based on microexplosions of water contained in the hard tissues of the tooth under the influence of laser irradiation.
If the tooth is too damaged and there is no way to restore it filling materials, then it is necessary to apply orthopedic treatment(artificial crowns, inlays).
The authors collected unstimulated saliva samples using the drainage method. However, the ability of these individuals' saliva was less effective compared to the saliva of individuals who did not have the syndrome. He considered the target population to be a group of children with Down syndrome aged six to eighteen years and their siblings. He found a 32% overall prevalence of dental caries. Children with trisomy 21 had a lower prevalence of dental caries than their siblings.
There was no significant difference regarding the salivary ion concentration of the two groups. Oral candidiasis - fungal infection, which affects people throughout their lives. Correct functioning immune system The human body usually favors an equilibrium between the autochthonous and host microbiota, but the physical, chemical, iatrogenic and mechanical changes that occur in the oral cavity can contribute to breaking the equilibrium established between the fungus and the host, resulting in candidal infections usually having an endogenous origin.
Prevention of caries
Search effective methods caries prevention is one of the main directions modern dentistry. Caries prevention consists of a set of measures and its effectiveness depends on the interaction of dentists and dental hygienists with the population.
Prevention includes:
Physicochemical changes in saliva, changes in pH and the concentration of sodium, calcium and bicarbonate ions among other substances appear to influence the survival of Candida in the oral cavity, which contributes to high concentration candida in the mouth of children with Down syndrome.
Classification by depth of lesion
In addition, children with Down syndrome experience impaired innate and acquired immunological responses beyond anatomical and physiological changes, macroglossia, salivary congestion due to oral incompetence, motor difficulties, making these additional factors more susceptible to infectious disease processes.
- Regular visits to the dentist at least once every six months.
- Carrying out professional hygiene oral cavity.
- Brushing your teeth at least 2 times a day.
- Application additional funds hygiene (gum rinses, dental floss, toothpicks, irrigators).
- Mouth rinse with remineralizing and fluoride-containing preparations.
- If the fluoride content in water is insufficient, it is necessary to compensate for the lack of fluoride by consuming fluoridated milk.
- The use of fluoride-containing gels for the prevention of caries.
- Dentists conducting hygiene lessons in schools and preschool institutions with demonstrations of teeth brushing techniques on models.
- Conducting lectures on oral care and risk factors dental diseases and their prevention.
- Drug therapy (fluoride tablets).





