There are five classes of defects in the hard tissues of teeth (carious lesions), differing in location. This classification was first proposed by the American dentist J. Black. It guides the preparation and selection filling material. There are V classes:
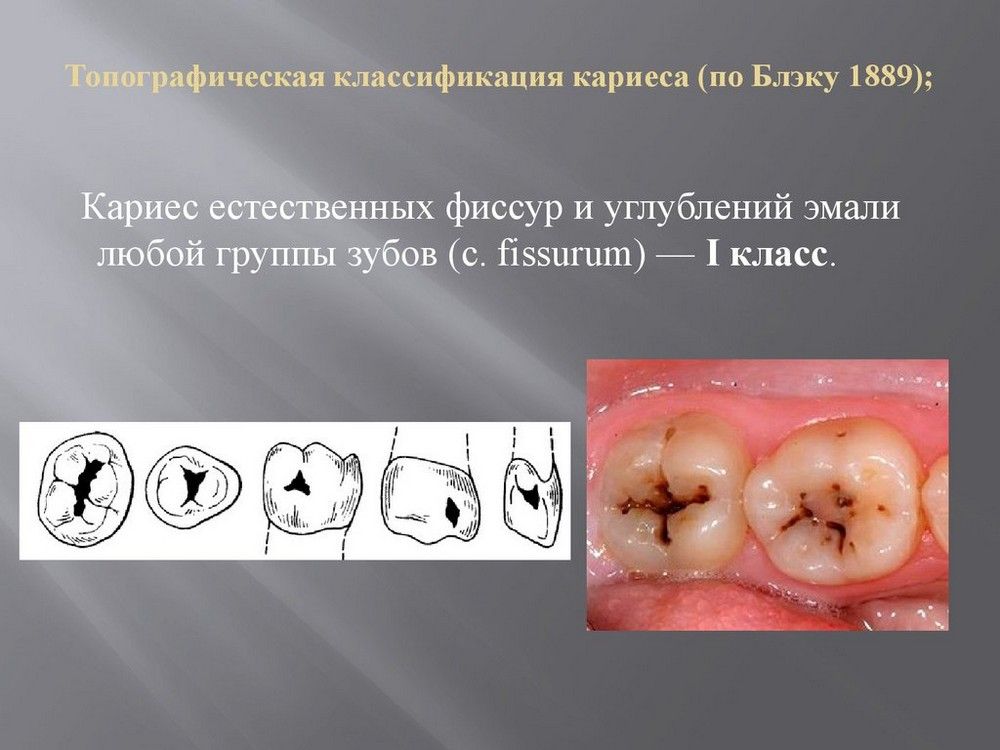
Class I - cavities are localized in fissures, in the blind fossae of molars, premolars, incisors and canines. Thus, according to the first class it can be on the occlusal, buccal or lingual surface.
Development of caries and its symptoms
It is an irreversible microbial disease of calcified dental tissues, characterized by demineralization of the inorganic part and destruction organic matter tooth Dental caries are the result of the formation of plaque, which contains bacteria, which in turn contains carbohydrate carbohydrates, available daily food products. This acid production in turn lowers the pH below 5. long-term exposure low pH leads to demineralization of the tooth structure with which it was in contact.

Class II - the cavity involves at least two surfaces: the mesial or distal and occlusal surfaces of molars and premolars. Thus, a second class filling can be located For example, on the mesial-occlusal surface (MO) of a premolar or on the mesial-occlusal-distal surface (MOD) of a molar.
Saliva acts as a neutralizing agent to raise pH levels, which can lead to remineralization in most cases. Classification of dental caries is carried out depending on the location of the carious lesion. This is also known as "early childhood caries" a common problem among children under five years of age, but can be avoided through awareness and prevention. If your child begins to exhibit symptoms, your dentist may provide treatment for baby bottle tooth decay.
The type of treatment depends on the severity of the breakup. As with most health problems, than problem before will be resolved, the less extensive and invasive the treatment will be. Treatment of baby lotus decay. Treatment varies depending on your child's age and the severity of the condition. At the most early signs problems, you and your child's dentist can work together to formulate an approach to management and treatment.


Class III - cavities are localized on the medial and distal surfaces of the incisors and canines.


Reasons for the development of the disease
White spots on the surface of the tooth are early symptoms baby bottle tooth decay, according to the North Dakota Department of Health. At this point, a fluoride treatment or fluoride varnish may be used to remineralize all teeth. This treatment actually reverses the decay by early stages, helping to restore surface enamel. Your child's dentist may also recommend fluoride supplements. At this stage, you can also make changes to your child's diet to continue to break down.
Class IV - cavities are localized in the same place as class III cavities, but with a violation of the angle of the coronal part of the tooth or its cutting edge

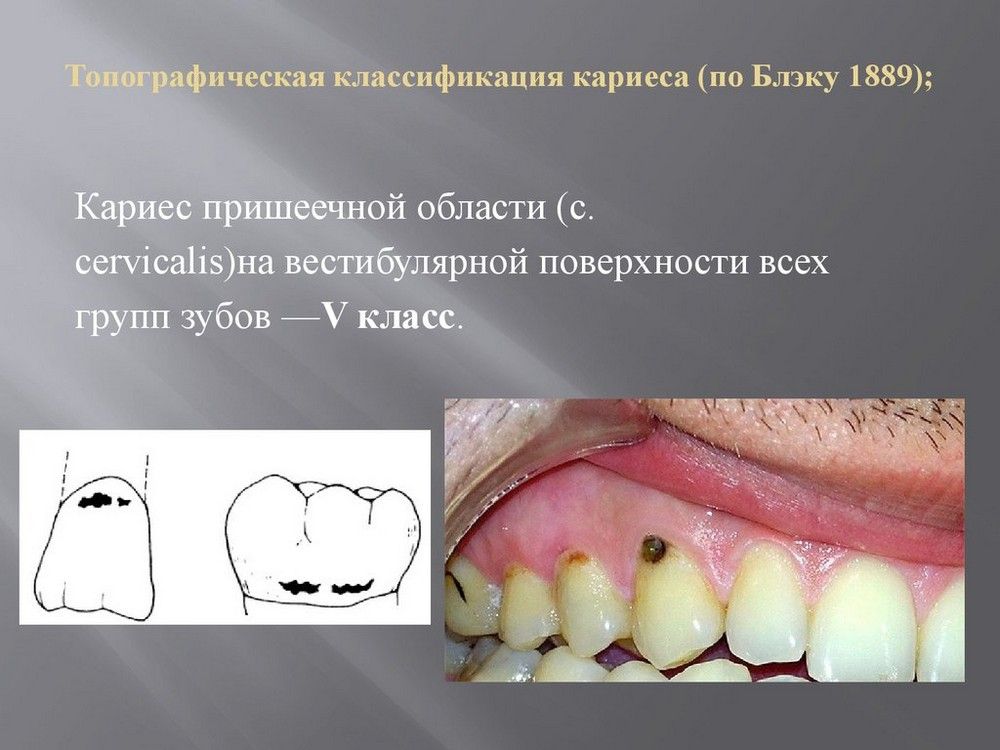
Class V - cavities are localized in the cervical region of all groups of teeth.
Thus, a fifth class filling can be located, for example, on the vestibular surface of an incisor upper jaw in the cervical region or on the lingual surface of the molar lower jaw in the cervical region.
Limiting acidic foods Limiting juices, especially citrus juices Substituting water for juice, formula or milk in your baby's bottle. Depending on the age of your child, general needs in health and nutrition, some dietary changes may be undesirable.
If the decay is noticed for more late stages, fluoride treatments will no longer be sufficient. Symptoms of more severe decay include.
- Brown or black spots on teeth.
- Bleeding or swollen gums.
- Fever, swelling, or irritability, which may indicate an infection.

Basic principles of preparation of hard dental tissues:
A permanent filling cannot be placed directly into a carious cavity. The cavity must first be prepared to ensure the following:
- All soft tissue was removed from the cavity carious dentin However, in some exceptional cases, the deepest pigmented but hard layer of dentin may be left in order to avoid accidental exposure of the dental pulp.
- The enamel, devoid of underlying dentin, is removed.
- The filling will last a long time.
- Secondary caries will not occur.
Basic principles of preparation carious cavities are as follows:
If your child's dental decay is severe. Treatment for baby bottle tooth decay is almost the same as for adult tooth decay. The American Academy of Pediatric Dentistry states that stainless steel crowns are often used because they are durable and less likely to require follow-up treatment or replacement. Your dentist may suggest sedation or even general anesthesia for extensive restoration work depending on the age and maturity level of your child. In very severe cases, it may even be necessary to extract the teeth.
- There should be no damaged tissue left on the walls of the cavity. Carious dentin and infected tissue are removed using an excavator or large ball bur at low speed. tip.
- The enamel, stripped of underlying dentin, is excised with a high-speed bur.
- Then, using a turbine and mechanical tip and burs of various configurations, a cavity is formed taking into account the retention of the filling and the resistance of the tooth tissue.
Most often, people go to the dentist with a complaint about caries. This disease is damage to the surface of the tooth, followed by softening of the deep layers of dentin. Untreated enamel damage can lead to tooth loss and provoke the development of various diseases.
This is most likely necessary if the tooth is infected or has become so badly decayed that it cannot be restored. The importance of treating baby lotus decay. It is a common misconception that premature loss of children's teeth is not a problem. Those teeth are going to fall out eventually anyway, so why worry if they fall out earlier than planned? In fact, there are many reasons to worry about the premature loss of children's teeth.
Classification by localization
Permanent teeth that will serve your child throughout adult life, present in the jawbone with early years your child. Children's teeth act as a placeholder for permanent teeth. If they are lost prematurely, the distance between permanent teeth Can Premature loss of children's teeth can cause permanent teeth to shift along with other problems that may require extensive orthodontic treatment.
Reasons for the development of the disease
The disease develops due to microorganisms in oral cavity, under the influence of which, together with saliva, the breakdown of food occurs. In this case, organic acids are formed. Lactic acid negatively affects the enamel; under the influence of this substance, the process of demineralization begins. Demineralization causes a small light spot to appear on the enamel. The spot is characterized by the first.
This may also affect his ability to speak correctly. Correct diction requires the presence of front teeth, so premature tooth loss may result in the need for future speech therapy. Poor hygiene habits can follow your child into adolescence and in adulthood. The best way Ensuring ongoing dental health as your child gets older means making sure he or she learns with good oral hygiene from the very beginning. Products such as toothbrushes and toothpaste, will help you introduce regular tooth brushing to your child.
If you do not consult a doctor in a timely manner, the demineralization process will continue and will first lead to the appearance of a depression (carious cavity), and then to a softening of the deep layers of dentin. When the process of dentin destruction has begun, careful treatment is necessary, otherwise there is a risk of developing pulpitis and periodontitis, as well as loss of a healthy incisor.
Determination of caries intensity
The best approach to baby bottle tooth decay is prevention. If your child does experience early tooth decay childhood, you and your child's dentist can work together to determine best options treatment. 
While most babies don't start getting teeth until they are 6 months old, dental care important from the very beginning. Many dentists recommend starting visits before your child's first birthday to ensure that the teeth and gums are being cared for and cleaned properly.
Treatment of the disease involves dissection of hard tissue. During preparation, the affected areas of dentin are removed and a filling is applied.
Classification of the disease
Caries is classified depending on the degree of damage to the enamel and the development of the carious cavity. At the same time, in dentistry there are several various classifications diseases:
Teething – Between 3 and 9 months, your baby's baby teeth will begin to erupt. Teething can make your baby irritable or fussy and cause fussiness, drooling or loss of appetite. In fact, sucking often provides comfort even after the baby no longer needs to breastfeed or bottle feed. Baby bottle tooth irritation - this occurs when acid is formed by bacteria on teeth, from sugar in food and drinks, damages tooth enamel, which causes demineralization and can eventually lead to a cavity. Nipples - Sucking is a normal part of development for children in the early years of life. . Today, caries remains one of the most common diseases throughout the world.
There are about 20 different classifications, but it is the ones listed above that have become widespread in dentistry with the approval of the WHO.
Black classification
A famous dentist from the USA, Black conditionally divided diseases into classes. Black's classification of the disease consists of 6 classes and allows one to distinguish the degree of enamel damage and the development of a carious cavity depending on the location of the process.
Dental caries, also known as tooth decay or cavity, is an infection, bacterial in origin, that causes demineralization and destruction of the hard tissues of teeth. It is the result of the production of acids by bacterial fermentation of food debris accumulated on the surface of the tooth. If demineralization exceeds saliva and other remineralization factors such as calcium and fluoridated toothpastes, these hard tissues gradually break down, producing dental caries.
The black classification of dental caries is standard method, used in identifying carious lesions depending on its location on the tooth surface. Blacks originally developed five classifications, but later added a sixth. These cavity classifications are used when recording on a patient's chart the type of caries found on the teeth.
Black's classification of caries describes the following classes:
Initially, Black's classification of enamel lesions included only 5 classes. The last, 6th grade, was added later at the initiative of WHO. This made it possible to supplement the classification and obtain a more detailed picture of the destruction of enamel and dentin.
How is dental disorder diagnosed?
Occlusal surfaces of molars and premolars. Occlusal two-thirds of the buccal and lingual surfaces of molars. Lingual surfaces of anterior teeth. The tooth preparation procedure involves removing defective or loose tooth structure. The shape of the outline should consist of smooth curves, straight lines and a rounded line and sharp corners. During tooth preparation, the edges of the preparation not only extend into the sound tooth tissue, but also include adjacent deep pits and cracks during the preparation process. This is done in order to prevent relapse of caries in the fields of fillings, where relapse of decay is most often observed. Factors influencing the shape of resistance: Amount of occlusal stress. Type of restoration used. Amount of tooth structure remaining. Limit expansion of outer walls to ensure strong marginal ridge areas with adequate dentin support. Incorporation of weakened tooth structure to avoid fracture under masticatory forces. Rounding the inner corner of the line to reduce stress concentration points during tooth preparation The shape of the resistance also depends on the type of restorative material used. For example, high copper amalgam requires a minimum thickness of 5mm, cast metal requires a minimum thickness of 0mm, and porcelain requires a minimum thickness of 0mm for fracture resistance. Composite and glass ionomer restorations are more dependent on the occlusal wear potential of the restorative area and typically require thicknesses greater than 5 mm. Resistance to tooth shape provided by a flat pulpal and gingival floor. In the case of a rounded pulp floor, the rocking motion of the restoration results in a wedge-shaped force that can lead to failure of the restoration. Typically, resistance and retention forms are produced to provide the same characteristics, so they are sometimes described together. General factors, affecting the form of retention are the following: The amount of masticatory stress applied to the recovery. Thickness of restoration. The total surface area of the restoration exposed to masticatory forces. amount of tooth structure remaining. The form of retention depends on the type of restorative material used: Amalgam: Retention increases with amalgam restoration in the following way: Ensuring occlusal convergence of dentin walls in relation to the tooth surface. Minor undercutting of dentin close to the pulp wall. Preservation of marginal ridges. Providing occlusal dovetail The wall preparation should have 2°-5° occlusal convergence to retain the amalgam. The dovetail helps in providing retention. Undercutting in dentin helps in retention of composites. In composites, retention is increased by: Micromechanical bonding between the etched and primed tooth structure and the composite resin. Providing enamel bevels. Direct gold filling: The elastic compression of dentin and the starting point in dentin ensure retention in direct gold fillings by proper condensation. Infected dentin must be removed even if it results in exposure to cellulose, which is treated accordingly. Cellulose protection is achieved using liners, varnishes and bases depending on: the amount of dentin thickness remaining the type of restorative material used. Liners, varnishes, bases: Liners and varnishes are used where the preparation depth is shallow and the remaining dentin thickness is more than 2 mm. They provide: Barrier to protect residual dentin and pulp Galvanic and thermal insulation. The bases are cements used on pulpal and axial walls of 5 to 2 mm thickness under permanent restorations. They provide thermal, galvanic, chemical and mechanical protection for cellulose. Commonly used base materials are zinc phosphate cements, glass ionomers, polycarboxylate cements, zinc oxide eugenol and calcium hydroxide. These are as follows: Grooves and Coves: Wherever there is volume of dentin, grooves are prepared without undermining the adjacent enamel. Coves are small conical depressions. The grooves are placed into prepared healthy dentin to provide additional axiofacial and retention. axiologically, as right angles to increase the retention of restoration slots or internal boxes: they are mainly used in amalgam restoration. They have a depth of 0 to 5 mm, such as grooves produced in dentin to increase the surface area. Pins: Used to provide additional retention Various types pins various shapes and sizes. They can be used in all types of restorations such as amalgam, composite and cast restorations. Skirts: Skirts are prepared to provide additional retention in casting restorations. They increase the total surface area of the drug. Skirts can be prepared on one of all four skirts on the cast sides of the restoration of the preparation depending on necessary assistance in increasing retention retention. Amalgampins: Amalgampins are vertical posts of amalgam cemented into dentin. Amalgampins increase retention and stability full recovery. Beveled enamel edges: The accumulation of preparation fields increases the surface area and thus supports composite restorations. Etching of enamel: Etching results in microscopic roughness, which increases surface area and thus favors dentin: Etching and priming of the dentin surface, done in some restorative materials, increases retention. Adhesive cementitious cements: Adhesive cementitious cements increase retention of indirect restorations. The finishing process further improves the design and smoothness of the cavour, which ensures maximum adaptation of the restoration to the walls and edges and maximum restoration efficiency. Wall preparation results in: Better marginal seal between the restoration and the tooth structure. Increased strength of both tooth structure and restoration at and near the margin. Strong field arrangement. Increasing the degree of smoothness of the fields. The degree of smoothness of the walls: depends on the type of restoration used. For example, for restorations from cast metal a very smooth surface is required, whereas direct gold, amalgam and composite restorations in the preparation walls require little roughness. Position of fields: during the finishing of walls and preparation fields, the principles of parallelism of the direction of the enamel wall should be followed. Knowledge of enamel cores is essential to properly finishing preparation fields. In margins, all enamel walls should have full length cores supported by dentin. Peculiarities finished drug: The design of the cavurus surface angle depends on the type of restorative material used. For example, for amalgam restoration, a 90-degree surface angle of the cap provides maximum force for restoring teeth. This includes removing debris, drying the preparation, and final inspection before placing remedial materials. Preparation of the preparation has the following purposes: Cleaning the preparatory walls, floors and fields from enamel and dentin chips that arise during the preparation of the tooth: Remove all residues from the preparation, especially on the margins, otherwise the residues on them will remain dissolved, resulting in the formation of microcooling, which can lead to secondary caries. Purification of the drug can be carried out using warm water. Stubborn debris can be removed using a small cotton ball soaked in water or hydrogen peroxide. Drying the tooth preparation before inserting restorative materials: This can be done using air, dry cotton pellets and commercial cleaners. It is important that the teeth do not become dehydrated by excessive use of air or hot air. Sterilization of the preparation walls using very weak disinfectant alcohol-free: use a mild disinfectant in . It is a defect in the structure of a hard tooth caused by abuse like tooth decay and trauma. What is dental preparation? This is the mechanical modification of a defective, damaged or diseased tooth to produce a restorative material that restores the health of the tooth, including its aesthetics, normal shape and function. Definitions Dental preparation, which refers to the restoration of amalgam, gold or ceramic, can be considered traditional preparations that require a certain shape, depth and marginal shape. Definitions. Tooth preparation for bonded direct restorations as composite or glass ionomer has less need for specific depth, wall and marginal shape and are considered modified preparations. Indications for restorative intervention: restoration of a damaged tooth. Restore your teeth with birth defects development. Replace the defective restoration. Need for improved shape or aesthetics. Why do we prepare carious cavities? To remove caries and create a compatible foundation for restoration. Determinants of cavitation preparation. Specific to a specific material. What are the basic principles on which cavities are prepared? What are the main stages of cavity preparation? Cavity Preparation Steps 1-Outline Shape 2 Resistance and Retention Shape 3-Convenience Shape 4 Removal of remaining caries 5 Completion of Cavity Walls 6-Toilet of Cavity 1-Outline Shape Defined as the Shape of the boundaries of the filled cavity External Contour Shape refers to the marginal boundaries. The inner shape of the contour refers to the shape internal form drug. Internal contour shape External contour shape Extension to the sound structure of the tooth. Avoid terminating fields at extreme heights, such as the height of ledges or the crest of a ridge. Rules for contour form. 4. Expand the preparation margin to include all cracks that cannot be repaired by enamel repair. Holding form holding form refers to design features there is a cavity in the preparation, which allows it to be securely held during function. 2. Resistance and form of retention. It describes those features in a prepared cavity that improve visibility and accessibility during preparation and restoration. This is the removal of any remaining infected decay left in the tooth after the initial preparation. In dentin, as the development of caries, the area of decalcification precedes the penetration of microorganisms. Infected carious dentin is removed alone, leaving a rounded, concave area in the wall. 4 - Removal of remaining caries. Hand cut. Mechanical excavation on the sides. Air purification from abrasion. Laser cleaning. The enamel rods forming the corner of the cavuroscope must have their inner ends resting on the sound dentin. The corner of the cavuroscope is beveled and covered strong recovery. 6 - Toilet the cavity The cavity must be clean and dry before placing the final restoration. It is designed to - remove debris, dentin chips, saliva. - Improve adaptation of the final restoration. - Prevent recurrence of decay This is done using air spray. References Chapter 7: Principles of Tooth Preparation Chapter 6: Fundamentals of Tooth Preparation.
- The outline form should include all defective holes and cracks.
- The initial preparation depth should be between 2 and 8 mm.
- Definitions What is a cavity?
Black classes are widely used in dentistry. Black also described the preparation of damaged teeth, which was later approved by WHO.
 Black's hard tissue preparation involves preparing the tooth before filling, since the filling cannot be placed directly into the damaged cavity. Preparation consists of several stages:
Black's hard tissue preparation involves preparing the tooth before filling, since the filling cannot be placed directly into the damaged cavity. Preparation consists of several stages:
- cleansing the incisor from soft dentin damaged by the disease;
- removal of damaged enamel;
- installation of a seal.
Such a filling will serve long years, wherein complete removal softened dentin avoids the development of secondary caries.
WHO classification
The WHO classification of caries of permanent teeth consists of several classes that characterize the disease depending on its location:

The WHO classification also takes into account unspecified types of caries, which can be complicated by other diseases of the oral cavity.
Based on the degree of damage, the following classes of caries are distinguished:
- a stain formed due to demineralization of the enamel;
- superficial lesion, in which the boundary between enamel and dentin is not affected;
- medium lesion, which affects the enamel and the upper layer of dentin;
- a deep form of the disease, in which the deep layers of dentin are affected and there is a risk of damage to the pulp.
Localization of the lesion
Classification of caries depending on location describes the following classes:

By danger possible complications, the disease is divided into two types - complicated and uncomplicated caries. An uncomplicated disease, according to WHO, does not lead to the development negative consequences. Complicated caries is running form a disease that over time destroys the pulp and can lead to the development of periodontitis.
Classification of lesions in children
In children who have not yet replaced their milk teeth with permanent ones, the development of caries occurs more rapidly than in adults. The classification of caries of primary teeth was given by Vinogradova; this systematization was subsequently approved by WHO and is used in modern dentistry.
Distinguish the following degrees lesions of baby teeth:
The decompensated stage of the disease is not always accompanied by demineralization of the enamel and the formation of pigmented areas.
Tooth preparation
Preparation of carious cavities involves complete cleansing affected dentin with subsequent installation of a filling. The procedure consists of several stages.

The preparation is accompanied by anesthesia. Anesthesia is necessary in cases that affect the pulp. Anesthesia is also indicated for patients with hypersensitivity enamels. For shallow caries, preparation is carried out without anesthesia.





