In addition to caries, there are a huge number of dental diseases. One of the most common pathologies is non-carious lesions of the enamel. Some of them have already been well studied in terms of symptoms, but some have not yet been finally sorted out. In this article, we will consider such a pathology as enamel hyperplasia. The development of such a pathology occurs in the process of laying and forming teeth in children.
What is enamel hyperplasia
The main manifestation of the disease is non-carious changes in the appearance of the tooth.
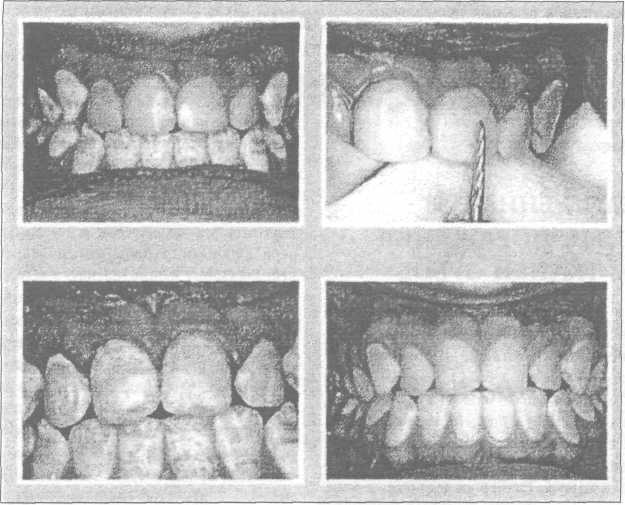
During the formation of teeth in children with this pathology, its excesses are formed, which appear as whitish convex islands. The overall functionality of the tooth remains normal, no discomfort does not cause disease.

Growths on the teeth - hyperplasia
It should be noted that this damage to the dental tissue is in no way associated with softening of the enamel with the participation of microorganisms. Hyperplasia is based on a violation of tooth mineralization under the influence of not only internal, but also external factors. In the presence of such a disease, even after its detection, only a third of all seek advice and help from a dentist.
General information and structure of enamel drops
Hyperplasia is a condition where excess tissue forms on the surface of a tooth. Pathology can develop both on milk and already on new teeth of a permanent nature.
Most often, the processes are formed in the basal part of the tooth or in the area of \u200b\u200broot growth. Hyperplasia or enamel drops are small in size from 1 mm, but in some rare cases can reach up to 5 mm. Such a violation is diagnosed in almost 2% of the world's population.
The only problem in diagnosing this deviation is an asymptomatic course.
The development of such small processes very often proceeds without any pain and therefore does not cause concern and desire to see a doctor. Most often, the problem lies in the unaesthetic appearance especially if the problem is centered on the front teeth.

Enamel drops on torn teeth
Dentists strongly recommend that if any deviations are found, even those that do not bring discomfort to initial stage development, seek advice and professional examination. Cervical hyperplasia is best removed on initial stage, because in practice it happens that such formations provoke the development of inflammatory processes in the gums.
Several types of enamel drops are determined by location:
- root;
- cervical;
- coronal.
By structure, hyperplasia is classified into:
- true enamel;
- enamel-dentine drops;
- enamel-dentine drops with cavities inside filled with pulp;
- drops of Rodriguez-Ponti, which are located in the periodontium in the form of nodular formations;
- drops are intradentinal, which are embedded in the dentin of the crown or the tooth itself.

Enamel drops on the edge of the tooth
Enamel drops that form in the dentin of the tooth cannot be diagnosed visually. Most often they can be found in the process of treating a tooth affected by caries. The bur machine accidentally hits a hardened area of dentin. Cervical hyperplasia is visible when probing the gums, and root hyperplasia can only be detected by the results of an X-ray examination.
You can treat only drops of enamel, which are located near the neck of the tooth.
The treatment process consists in polishing the tissue area with a diamond bur and subsequent daily care in the form of applying applications of fluoride toothpaste. Treatment continues for a week or 10 days on the recommendation of the attending physician.
Preventive measures to prevent the appearance of hyperplasia
Prevention of the development of dental hyperplasia in children consists in measures to prevent caries during the growth of milk teeth. It is also important to deal with complications that interfere with the normal formation of already permanent teeth. Every six months, take your child to the dentist so that he monitors the dynamics of tooth growth and conducts professional cleaning oral cavity.

Hyperplasia in advanced form
You can also try a procedure such as fissure sealing. composite material and a remineralization procedure.
Such activities will reduce the risks of developing any kind of enamel hyperplasia, and the baby's teeth will grow strong and radiate health.
To protect both an adult and a child from every adverse factor is simply an impossible task, therefore the main optimal way to combat the development of caries, hyperplasia, periodontitis and other maxillofacial problems is constant medical supervision. Starting with a woman who is preparing to become a mother, and then her child. Future mom becomes registered and observed from the 8th week of pregnancy and observation continues until the child reaches the age of two years. After that, the child is simply driven to scheduled inspection to a pediatric dentist.

Hyperplasia in a child - the initial stage
If the pregnancy is easy and the woman is not worried about problems with her teeth, then she must definitely visit the dentist 4 times. At the eighth, eighteenth, twenty-eighth and thirty-eighth weeks. The task of the dentist is to identify caries on early stage its development or periodontitis. Introduce a woman to preventive measures care of the teeth and the entire oral cavity, to teach the mandatory set of skills in personal hygiene. If diseases of the oral cavity are detected during pregnancy, then the number of visits to the dentist is prescribed on an individual basis and allows you to adjust the treatment until the moment full recovery future mother.
If the baby does not have problems with the oral cavity, then a dentist consultation is needed no more than once a year (up to three years). Then a dentist consultation is required every 6 months. When diagnosing tooth enamel hyperplasia, observation flows into a treatment process that lasts until complete cure teeth.
Reasons for the development of hyperplasia
Very often, such a deviation from the norm as hyperplasia is observed in connection with hormonal disruptions in organism. Such a cup most often ripens during puberty, during childbearing, with certain blood diseases and an excess of formed tartar. Sometimes the appearance of pearl drops is provoked malocclusion that injure the surface of the tooth enamel. However, the main reason is an insufficient amount fluoride in tooth enamel or its excess intake.

Forms of enamel hyperplasia
Treatment process
With the help of a drill, it is possible to cure cervical hyperplasia, which, in the process of growth and development, can provoke inflammation of the gums. Tooth drops are removed, after which the enamel is polished. Next, the dentist individually prescribes complex therapy medicines.
If a child is afraid of a doctor, then before going to a consultation, the baby should be prepared and told about the beauty of even and white teeth. He must understand that teeth are needed not only to eat, but also for beauty, to smile and everyone around him could see how beautiful and beautiful he is. healthy teeth. If there are uneven teeth in the mouth, then this is reflected in the pronunciation of words, in the bite and even in the shape of the face, which does not really decorate the guys. That is why you need to constantly go to the dentist, who helps all children to have beautiful teeth.

Enamel sealant is used in the treatment
The treatment process depends on the type of violation and the characteristics of dental pearls.
Another very important point- when the patient asked for help, namely, how advanced the disease is. Modern medical centers and innovative equipment make it possible to carry out treatment absolutely painlessly with minimal time and financial costs. Today you can get rid of hyperplasia quickly and efficiently. Sometimes the attending physician recommends additional orthodontic treatment. You may need, in addition to applications with fluorine and calcium, electrophoresis with calcium ions.
A good specialist will be able to diagnose hyperplasia at an early stage of its development, which will facilitate the treatment process and relieve gum problems.
It is important not only to identify the symptoms of the disease and prescribe effective treatment, but also to understand the root causes of the development of the anomaly in order to exclude them.
Unfortunately, even after successful treatment light spots on the enamel sometimes remain and such defects can be eliminated only through microprosthetics. But such a procedure is performed by a dentist, only to persons who have reached the age of majority, so all childhood will have to go through with unaesthetic defects on the teeth.

Treatment of timely detected hyperplasia
Important right from the start early age teach the child to properly care for their teeth and the entire oral cavity, so that in the future they will not lose permanent teeth ahead of time. It is recommended to start caring for the child's oral cavity from the very moment of his birth, even despite the fact of the absence of teeth. Often after breastfeeding, bacteria accumulate in the mouth of the baby, which leads to inflammatory processes on the mucous membrane. Young parents should monitor this and wipe the child's gums regularly. soft cloth dipped in warm water or a gauze swab.
Not only permanent teeth, but also milk teeth need careful care.
Because the correct laying and formation of permanent teeth depends on the condition of milk teeth, and diseases on temporary teeth can lead to deformations, unaesthetic problems.
It would be good if all parents understood that with the appearance of the first tooth in a baby, he needs to get his own brush, toothpaste and learn how to handle them. The main thing is to carefully approach the choice of products that will not harm the child.
Chapter6 Non-carious lesions of the teeth
In our country, a number of classifications of non-carious lesions of the teeth are known (V.K. Patrikeev; Yu.A. Fedorov and others).
In the International Classification of Diseases (ICD X revision, WHO), non-carious lesions of the teeth are represented by the following forms:
K.00.3. Mottled teeth (endemic /fluorous/mottling of enamel /fluorosis of teeth/; non-endemic mottling of enamel /non-fluorous opacification of enamel/; unspecified);
K.00.4. Tooth formation disorders (prenatal, neonatal enamel hypoplasia; cement aplasia and hypoplasia; dilaceration /enamel crack/, odontodysplasia; Turner's tooth; other specified; unspecified);
A 50.512. Hutchinson incisors;
A 50.52. Molars in the form of mulberries;
K.00.5. Hereditary disorders of the structure of the tooth, not elsewhere classified (incomplete amelogenesis, dentinogenesis, odontogenesis, dentinal dysplasia, shell teeth; unspecified);
K.00.8. Other developmental disorders of the teeth (discoloration during formation due to incompatibility of blood type, birth defect biliary system, the use of tetracycline; other specified disorders of dental development);
K.03. Other diseases of hard tissues of teeth:
K.03.0. Increased abrasion (erasure) of teeth (occlusal, contact surfaces; other specified; unspecified);
K.03.1. Grinding (abrasive wear) of teeth (caused by tooth powder - wedge-shaped defect, habitual, professional, traditional / ritual /; other specified; unspecified);
K.03.2. Tooth erosion (occupational, due to: persistent regurgitation or vomiting; diet; drugs; idiopathic; other specified; unspecified)
K.03.3. Pathological resorption of teeth (external /disturbed/; internal / pink spot/; unspecified);
K.03.6. Deposits on the teeth (pigmented plaque - black, green, orange; caused by the habit of using tobacco, chewing betel; soft white deposits; supragingival and subgingival calculus, plaque; other specified; unspecified);
K.03.7. Changes in the color of the hard tissues of the teeth after eruption (due to the presence of metals and metal compounds, bleeding of the pulp, the habit of chewing betel, tobacco; other specified; unspecified);
K.03.8. Other specified diseases of hard tissues of teeth (sensitive dentin, changes in enamel due to radiation; other specified). Taking into account this classification and domestic clinical classifications, the following division of non-carious lesions of the teeth is accepted:
I. Hereditary and congenital lesions of hard dental tissues:
1) anomalies in the size and shape of the teeth (merged, spiky teeth, macrodentia, microdentia, invagination of teeth, enamel drop);
2) mottled teeth - endemic mottling of enamel (fluorosis);
3) violations of the formation of teeth - enamel hypoplasia (prenatal hypoplasia, neonatal hypoplasia, Turner's teeth, Getchinson's teeth, molars in the form of mulberries, as a result of congenital syphilis);
4) hereditary disorders of the structure of the teeth - imperfect enamelo-, dentino- and odontogenesis;
5) other violations of the development of teeth (discoloration as a result of the Rh conflict, malformation of the biliary system, tetracycline intake).
II. Teething disorders and acquired lesions of their hard tissues:
1) violation of teething;
2) increased abrasion, including as a result of abrasive action toothpastes, powders, brushes, bad habits, occupational hazards and folk customs;
3) wedge-shaped defect;
4) erosion;
5) discoloration of the hard tissues of the tooth after eruption;
6) other damage to the hard tissues of the tooth - a change in the enamel as a result of radioactive radiation; dentine hyperesthesia.
III. Tooth injuries:
dislocation of the tooth;
fracture of the crown of the tooth within the enamel, dentin, opening of the pulp;
fracture of the root of the tooth.
In childhood, hereditary and congenital non-carious lesions of the teeth are mainly found:
1) enamel hypoplasia;
2) fluorosis;
3) drug and toxic disorders in the development of dental tissues;
4) hereditary disorders in the development of dental tissues. Much less often, non-carious lesions that occur after teething are found in children:
1) dental injuries;
2) drug and toxic disorders in the development of dental tissues;
3) increased abrasion of teeth.
Hereditary and congenital lesions of hard dental tissues
Anomalies in the size and shape of the teeth are described in section18 " dental anomalies". This group of hard tissue lesions includes enamel hyperplasia, which manifests itself in the excessive formation of tooth tissue. A synonym for enamel hyperplasia is "enamel drop" or "enamel pearl". Their origin is associated with the process of differentiation of the cells of the Hartwig's vagina into enameloblasts.
Enamel drops are more common in the region of the necks of the teeth, sometimes at the site of the bifurcation of the roots. Their size reaches 2-4 mm in diameter. In the clinic, they do not show themselves in any way and are found as an unexpected find. Cervical enamel drops are usually found on gingival retraction. (see section2) and exposure of the neck of the tooth, root - can be seen during X-ray examination or after tooth extraction.
Meanwhile, intradental (intradentinal) enamel drops are more common when the doctor, when preparing a carious cavity within the dentin, detects a harder part of it with a burr.
Only cervical enamel drops are subject to treatment. They must be ground with a diamond head and polished in this area of the tooth, and then the patient should be advised on daily applications of phosphate-containing toothpastes for 7-10 days.
Dental fluorosis is an endemic disease caused by fluorine intoxication, resulting from the consumption of drinking water with a high fluoride content during the formation of the dental follicle. One of the early signs of fluorosis is tooth decay. At a significant concentration of fluorine (above 5-10 mg / l), it is also affected bone skeleton man and animals.
The main source of fluoride is drinking water. The prevalence and intensity of dental fluorosis among the population increases with an increase in the concentration of fluoride in water. So, with a fluorine content of up to 0.5 mg/l, no changes in the tissues of the teeth are observed; at a fluorine concentration of 0.8-1.0 mg/l, mild forms of fluorosis occur in 10-12% of the population; at a concentration of 1.0-1.5 mg / l, fluorosis is observed in 20-30% of the population; with a fluorine content of 1.5-2.5 mg / l - at 30-45%; at a fluorine concentration of 2.5-3.0 mg/l - in 80-90% of the population. In areas with a hot climate, fluorosis can develop at a fluorine concentration in water of 0.5-0.7 mg/l, which is associated with its increased consumption. The presence of a significant amount of calcium in the water reduces the intensity of fluorosis.
Another source of fluoride in the body is food. The amount of fluoride in foods and beverages is largely dependent on the concentration of fluoride in the water used to prepare food and drink. In food, as well as in water, fluorine is found in an ionized form. However, food fluoride is absorbed worse than water-soluble fluoride. A large number of fluorine contains fish (especially cod), parsley, tea, walnuts, liver, beef
dina, cocoa. The level of fluorine is quite high in lamb, veal and oatmeal.
Another source of fluoride is fluoride-containing toothpastes. Despite the fact that the adsorption of fluoride in the oral cavity is less than 1%, there is evidence of a relationship between the frequency of enamel opacities (the initial degree of fluorosis) and brushing teeth with fluoride-containing toothpaste in the first two years of life (Sakharova E.B., 2001 and others).
The exact mechanism by which fluorosis occurs is not yet fully understood. More justified should be considered the idea of a hematogenous toxic effect of fluorine on enameloblasts during the development of the dental epithelial organ, leading to abnormal formation of enamel.
It is believed that fluorine, being an enzymatic poison, reduces the activity of phosphatase and, thereby, disrupts the mineralization of enamel. Yu.A. Fedorov et al. (1972) believe that fluorine, when administered orally and even locally, quickly penetrates and blocks, affects the activity thyroid gland. It is likely that altered thyroid function is the most likely explanation for the adverse effect of fluoride on enamel mineralization.
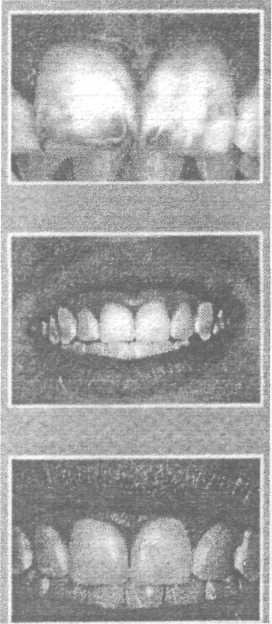
Teeth with fluorosis are called "speckled", "pockmarked enamel", "spotted enamel", "burnt" (Fig. 6.1; 6.2).
Foci of endemic fluorosis are characterized by a decrease in the prevalence and intensity of dental caries. However, the studies of Koshovskaya V.A. (1975) and Kovalenko L.I. (1977) indicate that caries in the endemic focus of fluorosis is affected not only by fluorine, but mainly by other macro- and microelements contained in drinking water and food products.
The most vulnerable period in terms of the possible development of fluorosis is childhood, namely, the period of mineralization of the tooth germs (from 3 months to 4 years) and the period of incomplete mineralization of the enamel in the first 1-3 years after the eruption of permanent teeth.
While most people living in the endemic focus of fluorosis have significant changes in the tissues of the teeth, some individuals have only mild lesions. Moreover, in such areas there are children whose teeth are perfectly healthy. This proves that the severity of dental fluorosis is determined by the degree of sensitivity of the body to fluoride intoxication and its ability to withstand this effect.
With fluorosis, symmetrically located teeth are affected, and the degree of manifestation of the disease is usually the same. The most pronounced clinical picture of this disease is observed on the central incisors and first molars, which is associated with the calcification of their crowns in the first year of life, when the child's body is significantly exposed to adverse environmental factors. Teeth, mi-
Rice. 6.1. Dental fluorosis. erosive form
208 ♦ Dentistry
Rice. 6.2. Dental fluorosis. Chalk-speckled form (according to T.P. Kroll)
Neralization of which takes place at an older age, are affected by a milder degree of dental fluorosis.
Depending on the severity of changes in the teeth with endemic fluorosis, the following clinical forms are distinguished (Patrikeev V.K., 1973):
- dashed form characterized by subtle chalk-like stripes on the enamel of the front teeth of the upper jaw;
- spotted form It is characterized by the presence of well-defined chalk-like spots located over the entire surface of the teeth. A feature of this form of dental fluorosis is that the enamel in the area of the stain is smooth and shiny. Sometimes there is a mild light yellow pigmentation;
- chalky (mottled) form manifests itself in the area of all, and not just the front teeth, is clinically very diverse: white shiny and matte spots, areas of pigmentation spots from light to dark brown. The spots are usually located on the vestibular surface of the front teeth. Sometimes there are small rounded enamel defects - speckles. With this form, there is a rapid erasure of the enamel with the exposure of dark brown pigmented dentin;
- erosive form characterized by more severe damage to the teeth and is accompanied by the formation of erosion defects in the area of chalky altered enamel;
- destructive form characterized by a violation of the shape of crowns due to erosive destruction and erasure of hard tissues. destructive form observed in areas with high content fluorine (10-12 mg/l) in drinking water. With this form, the tissues of the teeth are fragile, they are often broken off and, as a result, trauma to the oral mucosa.
Fluorosis of milk teeth is extremely rare (isolated cases are described), even in an endemic focus, and mainly on molars. This is due to the ability of the placenta not to pass an excess amount of fluoride to the fetus. The defeat of fluorosis of milk teeth is associated with early feeding of infants, or with an increased concentration of fluoride in breast milk.
Morphological changes in teeth affected by fluorosis are determined mainly in the enamel, more often in the surface
number of its layer. The structure of the enamel on the thin section appears to be sharply emphasized, which is explained by partial resorption of both enamel prisms and the interprismatic substance. As a result of the resorptive process, the enamel prisms themselves are less tightly adjacent to each other.
The Gunter-Schreger bands are sharply expressed, which curve in an arcuate manner and reach the enamel, the Retzius bands are clearly visible. The dentin-enamel junction has a serrated shape. The surface layer of enamel has a moiré pattern, which is due to an increase in interprism spaces due to partial resorption of enamel prisms, hypo- and hypermineralization zones.
Fluorosis at the spot stage is differentiated from caries, which is characterized by a single lesion in areas typical of caries. With fluorosis, lesions are multiple, located over the entire surface of the crown of the tooth and appear from the moment of teething. Mild manifestations of fluorosis may have a similar clinical picture with the spotted form. enamel hypoplasia. Severe forms of fluorosis, accompanied by the formation of erosions and other defects of the tooth crown, must be differentiated from caries, banal erosion, wedge-shaped defects, etc. (Table 6.1; 6.2).
Treatment. Therapy for fluorosis depends on the stage of the process. With a spotted and dashed form, a positive effect gives local treatment, the essence of which is whitening followed by remineralizing therapy. EV Borovsky (1978) recommends bleaching with solutions of inorganic acids.
Recently, acid etching of enamel during fluorosis is being replaced by grinding its surface by 20-70 microns. T.P. Kroll (1990) proposed a method for grinding off fluorescent spots using a paste containing hydrochloric acid, carborundum and silicon gel (Fig. 6.3 a, b, c).
With erosive and destructive forms of damage, accompanied by a violation of the integrity of the enamel, methods of restoring the shape and color of the tooth crown are used. Delayed filling with composite and filling materials is recommended after remineralizing therapy (general and local). It is also possible prosthetics with facings and crowns.
Non-carious lesions of the teeth♦ 209
Table 6.1 Differential diagnosis of caries and non-carious lesions occurring before teething
|
signs | |||
|
Enamel hypoplasia | |||
|
Time of occurrence |
After teething |
Before teething |
Before and after teething |
|
What teeth are affected |
Equally dairy |
Mostly permanent |
Mostly permanent |
|
and permanent | |||
|
Localization on the surface |
Fissures and pits, contact |
Symmetrical for namesake |
Atypical for caries throughout |
|
crown wear |
surface, cervical |
teeth. vestibular and lingual |
tooth surface |
|
area of teeth |
surfaces, tubercles of molars and | ||
|
premolars. | |||
|
The number and color of spots on |
More often single, cretaceous or |
More often single, cretaceous |
Multiple, chalky, yellowish |
|
brown |
to brown, indistinct line |
||
|
demarcation |
|||
|
Sounding results |
Defect surface |
The surface of the defect is dense |
|
|
rough | |||
|
Permeability to |
Increased significantly |
not enlarged |
|
|
dye | |||
|
The fate of the stain |
Disappear rarely, often in place |
Doesn't disappear |
May disappear with age. More often |
|
spots appear superficial |
does not change, slowly progresses. |
||
|
Damage increases |
Irrelevant |
Occurs in areas with |
|
|
drinking water |
with decreasing content |
high content of fluorine in |
|
|
drinking water. |
|||
Prevention. Preventive measures are divided into collective measures aimed at reducing the fluoride content in drinking water, and individual prevention measures. Reducing the amount of fluoride in drinking water can be achieved by replacing the water source or reducing the content through drinking water treatment techniques.
Individual preventive measures should be carried out from the moment the child is born. Artificial feeding and early introduction of complementary foods to the child should be avoided. With the introduction of complementary foods to the child, the main amount of water in food should be replaced with milk and juices. Additional intake of vitamin C, D, calcium supplements significantly reduces the manifestations of fluorosis. It is also necessary to take children out of the endemic area for the summer period.
Prevention and treatment of dental fluorosis should be carried out in a complex manner, taking into account the severity of the lesion, the general condition of the body and the influence of endemic factors. It should begin in early childhood and be carried out
systematically, using all available municipal and individual measures.
The overall impact on the body and teeth affected by fluorosis should include:
1) stopping or at least limiting the intake of high concentrations of fluoride with drinking water and food into the children's body. For this purpose, it is recommended to use water from a water source with a low fluoride content for drinking and cooking. In the absence of such an opportunity, partial defluorination of water is recommended by boiling it for 5-10 minutes, followed by settling.
The removal of children for the summer period from the endemic area is very important in the prevention of fluorosis. Clinical observations have shown that the replacement of water sources for 3-4 months annually in the first 8-10 years of a child's life contributes to the normalization of enamel formation and significantly reduces the percentage of teeth affected by fluorosis;
table6.2
Differential diagnosis of non-carious lesions
|
signs | ||||||
|
Superficial caries |
hypoplasia |
wedge-shaped defect |
acid necrosis |
|||
|
Short-term pain from chemical irritants |
Aesthetic defect, short-term pain from all irritants is possible |
Aesthetic defect |
Possible short-term pain from all irritants, can proceed painlessly |
Short-term pain from thermal and chemical stimuli |
||
|
Localization |
Fissures, pits, contact surfaces, cervical region |
Vestibular surface of incisors and canines in the middle third or throughout the crown |
Symmetrical, but atypical for caries. vestibular, lingual surfaces, tubercles of molars and premolars. |
Vestibular surface in the region of the neck of the tooth |
More often, the vestibular surface, the cutting edge of the front teeth, can be on any surface. |
|
|
Characteristics of the lesion |
Roughness, a defect within the enamel. The probe is delayed in the area of the defect |
Saucer-shaped defect, sometimes grooved, the bottom is hard, smooth. |
Defects in the form of small or large erosions, sometimes abrasion, enamel chips |
Small depressions in the form of dimples or grooves with a smooth surface |
Wedge-shaped defect with smooth bottom and walls |
Enamel loss, resembling increased abrasion. Sometimes the enamel takes on a chalky color |
Dentistry
Rice.6.3. Grinding of fluorous spots: a - fluorous spots on the central incisors; b - after grinding off the spots; c - 5 years after grinding (according to T.P. Kroll)
2) weakening the toxic effect of high concentrations of fluorine on the body as a whole and dental tissue in particular, by prescribing a rational diet. Restriction in the diet of dishes prepared from sea fish, strong brewed tea and other foods rich in fluoride. Recommended lean beef, pork, River fish. From dairy products - low-fat milk, cottage cheese. They are rich in calcium and low content fats are better absorbed by the body. For drinking, juices made from vegetables and fruits growing in another area are recommended;
3) the appointment of medications and the conduct of specific treatment is carried out by a dentist, taking into account the severity of the lesion and general condition organism. Given the competitive relationship of fluorine with calcium, one of the calcium preparations is prescribed orally: glycerophosphate or calcium lactate in age dosages 1 hour before or 2 hours after a meal. To weaken the ulcerogenic effect of calcium, before taking these drugs, you need to drink 3-4 sips of warm, sweet, weak tea.
All children living in the focus of endemic fluorosis are recommended to take drugs that increase the protective properties and resistance of the body (sodium nucleinate, potassium orotate, tinctures of Eleutherococcus, magnolia vine, multivitamins);
The oral cavity is a very vulnerable area human body, as it has its own microflora and is subjected to heavy loads every day. In addition to the common carious disease, hard dental tissues also attack other lesions that have received the definition of "non-carious".
Such pathologies differ in their individual symptoms and require unique methods treatment.
Types of pathologies
There are a number of pathological changes in the enamel that appear without the participation of pathogens, in particular cariogenic bacteria.
The classification of non-carious lesions of the teeth divides them into 2 groups: before eruption and after.

Enamel hypoplasia
Children's pathologies that have arisen in the process of follicular development and changes in tooth tissues include:
- hyperplasia and hypoplasia of enamel;
- endemic fluorosis;
- pathological eruption (change in the position of the tooth, its structure, enamel color, etc.);
- genetic and birth defects.
After eruption damage is possible not only to the rudiments, but also to hard tissues and dentin of the tooth. These pathologies include:
- increased wear and tear bone tissue tooth
- tissue erosion;
- death of tooth tissue (necrosis);
- abnormal pigmentation of the enamel, the appearance of soft microbial plaque and dark stone
- wedge-shaped defect;
- mechanical injury;
- hyperesthesia ( hypersensitivity) enamel.
hypoplasia and hyperplasia
Hypoplasia is a malformation of enamel due to a metabolic disorder in adjacent tissues and tooth rudiments. The pathology is irreversible and untreatable.
Visually, the disease looks like a series of multiple spots, deformations and depressions on the surface of the tooth. The size, shape and depth of the lesion is different. Sometimes doctors note the underdevelopment of the enamel at the bottom of the cavities or on the protrusions of the chewing surfaces.
The shade of spots is observed in light colors: white and transparent, yellowish. The edges of the lesions are well-defined, and the size is symmetrical to a similar tooth on the other side of the row. The surface of the defects is smooth, it can be glossy or matte, depending on the degree of mineralization disturbance.
Treatment of the disease involves the restoration of metabolism in tissues and normalization of mineral metabolism. Topical treatment is also applied with a 75% paste based on the sodium fluoride element. The agent should be rubbed into the affected surface. In dentistry, the enamel is opened with a fluorine-containing varnish, which protects the enamel from damage and produces a remineralization effect.

Non-carious lesions of the teeth
Hyperplasia also refers to non-carious lesions of the teeth that occur before teething. In this case, the disease provokes excessive mineral metabolism in the rudiments of future teeth, which in turn causes excessive development of hard tissues (the so-called "enamel drops"). Lesions are noted in the cervical and root region of the tooth.
Visually, the defect resembles a tubercle or a rounded protrusion, which looks like a drop. It consists of the enamel itself, as well as a layer of cement or dentin, inside which there is an area of pulp.
The symptomatology of the disease is not established, as well as functional disorders, that is, hyperplasia is considered more of a visual pathology.
endemic fluorosis
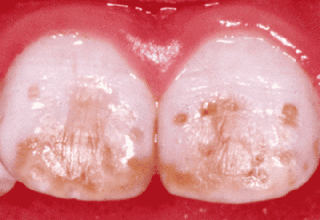
This disease is characterized by increased enamel pigmentation, the appearance of characteristic chalky spots on it. The lesion is caused by a high (more than normal) content of fluoride in the patient's body, which is usually associated with the structure of drinking water in certain populated regions.
The disease often occurs with early years of life when a child consumes fluoridated water.
Light spots are characterized by a matte structure and dullness, they look lifeless, which is associated with a violation of light refraction in the enamel. If the concentration of the element is exceeded to 1.5-2 mg per 1 liter, the formation of multiple yellowish or even dark brown spots is likely. Visually, the lesion creates a picture of rotten, neglected crowns.
Medicine defines several types of fluorosis, while some are accompanied by a change in the shape of the crowns, the appearance of multiple erosions, zones of abrasion and fracture of the tooth. Also, damage can reach the dentin.
To prevent the development of the disease in populated regions, the concentration of fluorine in running water is reduced. To do this, water sources are replaced, the waters of several channels are mixed, or water treatment plants are built that produce water defluorination.
![]()
Dental fluorosis
Parents should limit artificial feeding of infants, as well as early complementary foods, if the family lives in an endemic focus. If it is necessary to transfer to complementary foods, replace water with milk, industrial juices, order purified water from other regions.
Also, for the prevention of fluorosis, it is important to organize proper nutrition for the whole family. The diet should include enough protein foods, vegetables and fruits, natural juices, vitamins of groups B, A and C. The intake of phosphorus and calcium salts is beneficial. Food items should be excluded from the menu. high level fluorine - fatty species meat, sea and ocean fish, butter, strong tea.
With regard to oral hygiene, you should use calcium glycerophosphate-based toothpastes, which also do not contain fluoride components.
Treatment involves grinding the enamel and, if necessary, filling defects with photopolymer composites.
Abnormal development and eruption of teeth
Among non-carious lesions of hard tissues of the tooth, pathologies of eruption are noted. individual elements row. The disease is associated with initially incorrect placement of the rudiments, delayed development and eruption, fusion of the roots of several teeth. Often the defect is accompanied pericoronoritis, inflammatory processes in soft tissues.
Sometimes we are talking about premature eruption, which is caused by acceleration during jaw development. Such milk teeth are subject to amputation.
Among the pathologies, supernumerary teeth are also noted ( irregular shape, located additionally in the dentition or outside it), as well as adentia (incomplete dentition, partial absence teeth).

wedge-shaped defect
Changes in the pigmentation of milk teeth are associated with hemolytic disease of the newborn. Bilirubin accumulates in hard tissues and causes them to stain in different shades, including green, yellow, blue and purple.
Hereditary factors can also cause pathological changes cells, which affects the formation of dentin. Such disorders are the result of genetic pathologies (Lobstein-Frolik disease) or birth defects(dysplasia).
Treatment of this group of diseases involves overlapping crowns modern materials(porcelain, metal, etc.), the use of orthopedic structures (prostheses, braces, etc.).
Pathologies developing on formed teeth
Below are the main forms of non-carious lesions of the teeth that occur after eruption (starting from preschool age).
- enamel pigmentation, the presence of hard stone or soft microbial plaque. Deposits are represented by foreign elements that differ in color and structure. Soft plaque is formed due to the functioning of the microflora of the oral cavity and, in the absence of treatment, hardens, forming a dark stone. This pathology is primarily associated with poor hygiene oral cavity. Sometimes deposits are the result of the vital activity of fungal and viral microorganisms.
Enamel pigmentation occurs under the influence of endogenous factors. A pink tint can be seen after certain forms of influenza or cholera, yellow after jaundice, grayish-yellow spots appear after a long course of tetracycline antibiotics. The dullness of the enamel can also manifest itself in the case of the death of pulp tissue., putrid decomposition of dentinal canals. Among exogenous factors that affect the shade, we can distinguish food and medicinal pigments, tobacco tar.

Erosion of tooth enamel
- Increased tooth wear. It is a consequence of daily chewing loads. There is age and premature. Premature wear of crowns is associated with an incorrect structure of the jaw, wearing prostheses and implants, and an illiterate diet (the predominance of rough and fibrous food).
- wedge-shaped defect. There is an assumption that its appearance is influenced by problems with the endocrine, nervous, cardiovascular and digestive systems, encephalitis. Complications of the disease are exposure of the tooth necks, retraction of the gingival margin, and increased sensitivity of the enamel. Treatment involves taking vitamin and mineral complexes to strengthen the enamel, reducing its sensitivity. Topical treatment with glycerophosphate and calcium gluconate is also prescribed. In cases of deep defects, filling of cracks or even the installation of artificial crowns is prescribed.
- enamel erosion. In the presence of this pathology hard tissues teeth are gradually depleted and destroyed. The process is accelerated by the regular intake of acidic and salty foods, the use of hard brushes and tooth powder for hygiene. Also, the disease can be affected by thyroid dysfunction, mental and nervous disorders, gout.
All of these diseases begin asymptomatically and may long time do not disturb the patient. To prevent their development and expensive treatment in the future, visit the dentist at least once every 4-6 months for a preventive examination.
Caries with all its accompanying complications is the undisputed leader among dental diseases. Approximately 90% of visits to dentists are associated with carious processes. Non-carious lesions of the hard tissues of the tooth are much less common, but cause no less trouble. The pathogenesis of some non-carious lesions has not been fully elucidated, it is only indisputable that defects are formed without the participation of pathogenic microflora. However, bacteria with great pleasure join the process of tooth decay and the already existing pathological process exacerbated by caries.
Prices for the treatment of non-carious lesions
Treatment of non-carious lesions of tooth tissues 4032 P
Specialists in the treatment of non-carious lesions

Litvin Irina Borisovna
doctor of the highest category dentist-therapist1991 - graduated from the Moscow State University of Medicine and Dentistry. Semashko specializing in dentistry.
1991-1992 - passed a clinical internship on the basis of the Zelenograd city polyclinic, specializing in therapeutic dentistry.
1995 - graduated from advanced training courses at the faculty of advanced training of dentists of the Ministry of Health of the Russian Federation.
Non-carious lesions of hard dental tissues are divided into two groups:
- Arising at the stage of development of dental germs;
- Developing teething field.
The first group includes fluorosis, enamel hyperplasia, local and systemic hypoplasia, anomalies in the structure and development of the dentition. Some diseases are genetically determined, some are due to adverse effects on the rudiments of teeth during fetal development or in early childhood. To such unfavorable factors include diseases of the mother during pregnancy, taking certain drugs, especially the ecological situation in the region. After eruption, under the influence of chemical, mechanical and other environmental factors, erosion and wedge-shaped enamel defects, necrosis, hyperesthesia, pathological abrasion teeth. This group also includes injuries.
The classification according to ICD-S, developed on the basis of ICD-10, looks a little different. Due to radically different mechanisms of pathogenesis, anomalies in the development of teeth and actually non-carious tissue lesions belong to different groups. The most common non-carious lesions of the teeth Hypoplasia (underdevelopment) of the enamel. Enamel hypoplasia can be local or systemic. Systemic hypoplasia is a consequence of protein metabolism disorders and mineral salts, local - against the background of certain diseases and an inadequate diet. Sometimes enamel hypoplasia has a traumatic origin. The defect looks like cup-shaped spots or grooves on the surface of the tooth. Occasionally found complete absence enamel layer - aplasia. In our clinic, the defect is corrected by the method of microprosthetics.
A few videos about non-carious lesions of the teeth
The main types of non-carious lesions of the teeth
Photos with examples of non-carious lesions








In the photo, necrotic lesions, wedge-shaped defects and erosion look very similar, put accurate diagnosis only a specialist can. The ICD-10 classification also includes other pathologies of hard tissues of the tooth, but many of them are extremely rare. The cost of treating a specific defect is calculated on an individual basis, taking into account the prices of materials and the volume of intervention.
Prevention of enamel hypoplasiaTo prevent systemic hypoplasia, it is necessary:
- take care of the health of a pregnant woman and a newborn;
- to prevent infectious diseases and noncommunicable diseases in children;
- timely, qualitatively to treat the arisen diseases;
- to carry out sanitary-educational work in women's consultations, children's institutions, constantly work in contact with pediatricians;
- to prescribe npeparat tetracycline strictly according to indications.
For the prevention of local hypoplasia, it is important timely treatment or delete milk tooth so that inflammation from the affected milk tooth does not spread to the follicle permanent tooth.
Prevention of fluorosis
Fluorosis prevention consists of social and individual activities. Public events include:
- replacement of the water source;
- mixing of several water sources;
- defluorination of water (defluorination is carried out by chemical cleaning using alumina sulphate or passing through bone filters). Individual prophylaxis.
Prevention of fluorosis should begin from the moment the child is born until the end of the enamel mineralization period. It is necessary for a child breast-feeding. Children are recommended a sufficient amount of milk, vitamins (B1 B6, C). Additionally, calcium gluconate is prescribed. It is recommended to brush your teeth with toothpastes that do not contain the element fluorine. The food should not contain foods that contain fluoride. It is recommended to use imported products that are produced in areas with a lower content of fluorine in water and soil.
TO individual methods prevention of fluorosis include boiling drinking water, settling and drinking thawed water. In order to prevent fluorosis, it is necessary to take children out of areas where drinking water contains an excess amount of fluoride. During the school holidays, they can be taken to children's health camps, sanatoriums.
Prevention of wedge-shaped defect
In order to prevent a wedge-shaped defect, rational oral hygiene is recommended, in which teeth should be brushed with a soft brush and only toothpaste, and not tooth powder. Moreover, it is necessary to exclude horizontal movements with a brush while brushing your teeth. Recommended toothpastes: Zhemchug, Arbat, Fluorodent, Cheburashka, etc.
Prevention of tooth erosion
Prevention of tooth erosion consists of limiting the consumption of acidic foods (citrus fruits) and rational dental care. It is recommended to brush your teeth soft brushes, apply pastes containing glycerophosphate and other trace elements.
Prevention acid necrosis
Prevention of acid necrosis is proper organization production processes. First of all, there should be sufficient supply and exhaust ventilation, automation of acid production and process sealing should be established.
All workers chemical industries should be taken to the dispensary. In progress dispensary observation they need to conduct courses of remineralizing therapy 2 times a year. In order to prevent the development of acid necrosis, it is necessary to install columns with alkaline water for rinsing the mouth. Workers in chemical industries should rinse their mouth after 1.5-2 hours to neutralize the resulting acid compounds in the mouth.
Author: Muravyannikova Zh.G.
We advise you to read
 How to choose a taxation system for an LLC depending on the field of activity?
How to choose a taxation system for an LLC depending on the field of activity? Does an employer have the right to fine an employee?
Does an employer have the right to fine an employee? We draw up a business plan: how to open an atelier for tailoring and repairing clothes from scratch
We draw up a business plan: how to open an atelier for tailoring and repairing clothes from scratch Profitable business idea - babysitting services Business plan babysitter for an hour
Profitable business idea - babysitting services Business plan babysitter for an hour

