| Types of pin structures | 1. Pin teeth, in which the supra-root part is in contact with the tooth stump (Logan, Davis) | 2. Pinned teeth, in which the mouth of the root canal is closed with an inlay (according to Tsitrin, Ilina-Markosyan) | 3. Pin teeth, hermetically closing the tooth stump not only with a supraroot plate, but also with a ring (according to Richmond, Akhmetov) |
| Requirements for the root | The root must be at the level of the gum and be sealed to the top | The root of the tooth is at the level of the gum and is filled to the top | The root should protrude 1.5-2 mm above the gum and be sealed to the top |
| Indications for the use of pin structures | Complete destruction of tooth crowns upper jaw | ||
| Contraindications | Deep bite, discrepancy between root length and crown |
Educational situational tasks
1. To the clinic orthopedic dentistry A 56-year-old patient presented with a missing 11th tooth. The remaining teeth are intact. In the medical history, he was discharged from the hospital two weeks ago after suffering a myocardial infarction.
2. If during an examination the doctor suspects that the patient has syphilis, what should he do?
Your tactics for patient management.
Literature
1. Gavrilov E.I., Oksman I.M. Orthopedic dentistry. - 1978.
2. Gavrilov E.I., Shcherbakov L.S. Orthopedic dentistry. - 1984.
3. Kopeikin V.N. Orthopedic dentistry. - 1988.
4. Gavrilov E.I., Shcherbakov A.S., Trezuboe V.N., Zhulev E.N. Orthopedic dentistry. - 1994.
5. Abolmasov N.G. Replacement of defects in teeth and dentition with fixed dentures. - 1995.
6. Lectures from the Department of Orthopedic Dentistry of SOGMA.
METHODOLOGICAL DEVELOPMENT FOR LESSON No. 14.
Lesson topic:"Complete destruction of the crowns of single-rooted teeth. Treatment with pinned teeth. Types of pinned teeth, their features (Logan, Davis, Richmond, Ilina-Markosyan)."
Purpose of the lesson: study the indications for the use of various designs of pin teeth, their design features.
Structure practical lesson
| Stages | Providing classes | Time | |
| practical lesson | technical | teaching aids, | carrying out |
| equipment | controls | (min) | |
| 1. Organizational moment | Lesson plan, | ||
| educational journal | |||
| 2. Testing background knowledge | Tables, mula- | Slides, tasks | |
| live, phantoms | |||
| 3. Analysis of the topic of the lesson | Slide projector, | LDS, OOD, tests | |
| medical | |||
| tools | |||
| 4. Demonstration of the patient | |||
| 5. Independent work | |||
| 6. Control of results | |||
| assimilation | |||
| 7. Homework |
Review questions
1. Features of the structure of the upper and lower jaw.
2. Teeth, dentition and their structure.
3. Morphological and functional characteristic separate groups teeth.
Questions to check knowledge on the topic of the lesson
1. Indications for the use of pin teeth and requirements for them.
2. Pin tooth according to Richmond, Indications for use. Components and sequence of its manufacture.
3. Pin tooth according to Ilina-Markosyan. Indications for use and sequence of its manufacture.
4. Logan-Davis pin tooth. His design feature. Indications for use.
Pin teeth- These are permanent prostheses that completely replace the crown of a natural tooth and are strengthened in the canal of its root using a pin.
Pin designs are shown:
1) in case of significant destruction of the coronal part of the tooth, when it is not possible to restore it with a filling, inlay or crown;
2) to replace anterior teeth located outside the dental arch. In such cases, the teeth are depulped and their crowns are cut to the level required for the chosen pin tooth design.
The pin tooth must meet the following requirements.
1. Should not injure the tissues surrounding the root.
2. It should fit tightly to the surface of the root and thereby well isolate its canal from contact with the moisture of the oral cavity;
3. Should be well fixed to the root with a pin.
4. The pin should enter the canal 2/3 of its length.
5. Must meet aesthetic requirements.
6. Should not interfere with the closure of the remaining teeth and the chewing movements of the lower jaw.
Pin tooth according to Richmond.
The remains of the crown are processed in such a way that the root is at the level on the vestibular side, and on the oral side - above the level of the gingival margin by 1-1.5 mm and parallel to it. The diameter of the root is measured using a loop of thin wire with a diameter of 0.3-0.4 mm. Having removed the loop from the root, it is cut, the wire is straightened and a strip of the required width is cut along its length from the gold plate. Using pliers, a ring is made from the strip, the edges of which are closed and soldered with solder. Then the ring is fitted to the root, its edges are contoured along the neck of the tooth and moved under the gum by 0.3 mm. To obtain a protective mouthguard for the root, a gold plate is soldered to the ring and a cap is obtained that fits exactly to the circumference of the root. A hole is made in the cap for the pin. The pin is inserted into the root canal, the cap is put on the root; an impression is taken. The cap and pin are soldered. Then impressions are taken: working (with a pin and cap) and auxiliary. The models are plastered in an occluder. Selected according to the existing gap, shape and color, the porcelain tooth is ground to the vestibular edge of the cap along the incisal edge. The oral surface of the tooth is then modeled in wax, cast in gold and soldered to a cap.
After this, the porcelain lining is fixed to the gold protection using clamps with phosphate cement.
V.N. Kopeikin modified the production of a pin tooth with a ring in relation to chromium-nickel steel. Instead of a soldered gold cap, a steel cap is stamped onto the root. After fitting the cap, a pin is inserted through the hole made into the root canal, which is soldered to the cap. Then a monolithic or veneered part of the tooth is made.
Positive qualities pin tooth according to Richmond:
It is used for thin walls of the tooth root, strengthening them with a ring;
The cap prevents saliva from entering and decementing the pin structure.
Negative side: Often the metal in the area of the tooth neck is visible or the color of the plastic quickly changes.
Pin tooth according to L.V. Ilinoi-Markosyan.
The production of a pin tooth is carried out in several stages. During the first visit, the stump of the tooth root is prepared and a cavity is formed for the inlay. Then the root canal is prepared, after which softened Lavax wax is taken and pressed into the cavity, while a protective plate is modeled. Next, a pre-fitted pin made of clasp wire with a diameter of 1.0-1.2 mm is heated and inserted through the insert into the canal. After the wax hardens, the pin and inlay are removed from the cavity; In the laboratory, wax is replaced with metal.
Ilyina-Markosyan sought to eliminate the disadvantages inherent in the Richmond pin tooth. She suggested replacing the ring with a tab, which she calls a “shock absorber” or “retainer.” It is proposed to make the tab in cubic, square or oval shape. The cast protective plate and inlay fit tightly to the walls of the cavity and the root stump. The insert reliably fixes the structure in the canal and absorbs the lateral shocks that occur during chewing. Chewing pressure is evenly transmitted through the tab and the supra-root protective plate to the entire surface of the root.
Chewing pressure is transmitted through the entire root surface; there are shock-absorbing properties;
The inlay prevents cement resorption.
Negative properties: It is impossible to use this design with thin walls of the tooth root. The root may split under horizontal load.
Logan-Davis crown consists of a standard porcelain crown with a post hole and a metal post.
First, a crown is selected that matches the color, size and shape of the natural tooth of the same name on the opposite side. The crown is fitted to the root of the tooth so that the transition of the natural tooth into the crown is not visible from the vestibular side. In addition, the crown must fit tightly to the root stump, reliably isolating the entrance to the root canal from the penetration of oral fluid. Then the pin and crown are connected, as well as fixation with visphat cement.
LDS. Complete absence(destruction) of the tooth crown (2nd lesson)
Outline of Indicative Framework for Action (IFA)
| Sequence of student actions | Tools and means | Criteria, methods of control |
| 1. Preparation of the root canal for the manufacture of a pin tooth according to Ilina-Markosyan | Dental unit, handpiece, instrument set | Estimation of the length of the intra-root part and thickness of the root walls |
| 2. Preparation of the supragingival part and modeling of a cubic inlay | Diamond socket set, Lavax modeling wax, standard pin | Assessment of the ratio of intra- and above-root parts |
| 3. Fitting the inlay and taking an impression for occlusal protection | Set of carborundum stones, gypsum | Evaluation of fixation of the inlay with a pin in root canal |
| 4. Fixation of a pin tooth with phosphate cement | Tray with tools, spatula, glass, cement | Evaluation of a pin tooth in the oral cavity |
The crown part of the tooth, consisting of dentin covered with enamel, is its visible component, which rises above the gum and is directly involved in chewing food. Possibilities modern dentistry make it possible to restore the crown part of a tooth in several ways, depending on the extent of its damage.
Why does a tooth decay?
Every day, being exposed to significant stress, exposure acidic environment and the attack of millions of different microorganisms, our teeth get sick and slowly deteriorate even with the most careful care. Sooner or later, most of us are faced with caries and its disastrous result - partial or complete destruction of enamel and dentin.
Expert opinion. Dentist Voloshin O.L.: “Dentin is destroyed very quickly. It is enough to ignore a small carious hole, a notch or a slight chip on a tooth, and in a month a piece will break off from it larger size, and in six months 40-60% of the surface will be destroyed. But you don't have to ignore it proper care and regular visits to the dentist to get unpleasant surprise in the form of a broken tooth."
The following may also be the reason for this: factors:
- an internal, imperceptibly corroding tooth - it is hidden from prying eyes and is discovered only after the tooth crumbles literally before our eyes,
- sudden weight loss,
- unbalanced diet,
- periods of pregnancy and lactation.
- diseases urinary system and gastrointestinal tract.
- strong blow, fall, accident, other injury.
In addition to the nature of the damage, when choosing a restoration method, the decisive factor is which tooth will be restored - anterior or molar.
Restoring a damaged tooth with composite materials
The composite hardens under the light of a special lamp.
This is the easiest and most cost-effective way to get your teeth in order, but, unfortunately, it is not always suitable for use. It is permissible only when a small part of the crown has been destroyed - no more than 25-30% of the total surface, otherwise the filling will not hold well and will not last long.
Dentist performs composite extension in several stages: first expands the cavity of the hole and, if necessary, cleans out carious lesions. Important has the condition of the pulp and nerve, which determines whether a decision on depulpation will be made.
If for some reason it is difficult for the doctor to objectively predict whether the nerve will cause concern to the patient, he will first place a temporary filling, which will allow the patient to “test” the diseased tooth. In this case, the recovery process will take several visits. The next step is the formation of the coronal part using a composite. For front tooth restoration recommended light composite- this is a type of material that, in terms of light refraction, approaches natural dental tissues, and therefore practically does not stand out in the general dentition.
This type of filling material is durable, non-toxic, and comes in a wide range of colors. A special feature of the light-composite mass is that it hardens exclusively under the influence of ultraviolet light - this allows the dentist to take his time with the restoration process and form a crown that is anatomically close to the natural shape of the tooth.
This is what the pin structure looks like.
- The ability to reconstruct a tooth even with one wall and avoid its removal.
- 100% biological compatibility with human tissues.
- Hypoallergenic.
- Affordable price.
- Strength, thanks to which the structure will last at least 9-16 years.
- High aesthetics of the final result: metal-ceramic crown By appearance completely indistinguishable from natural teeth.
A necessary condition for prosthetics is good preservation of the roots and neck - if this is not met, the damaged tooth must be removed.
Tooth root restoration
What to do if the roots of the tooth are well preserved, but the destruction of the coronal part is too great and the orthopedic dentist is not sure what he can do increased load in the form composite material and a metal-ceramic crown?
In this case, the roots are restored using. The most popular prosthetics using anchor pin: it allows you to strengthen the entire dental structure and extend its service life. The anchor pin is installed on a special glass ionomer cement that holds it in the hole.
It is also possible to strengthen fiberglass pin– this procedure is used much less frequently due to its high cost. The advantage is that fiberglass is characterized by increased strength, and the disadvantage is that this material is completely invisible on x-rays. This property can create difficulties in the treatment of various dental problems.
The installation of a pin can be used as a safety net even if the damage does not require prosthetics, but has an area slightly beyond the maximum permissible (35-45%). In this situation, it will serve as the basis for reliable fastening of the light-composite material.
Stump inlays and onlays
Small defects in the front teeth can be corrected with veneers.
This method of restoring the crown of a tooth, such as installation, has long become popular. These are a kind of microprostheses - something between a pin and a filling. They are installed in the root canal and eliminate small defects resulting from caries. The inlay is made from metal according to individual parameters and takes several days, after which it is attached using a composite material.
Frontal overlays - veneers (read more about veneers) - are used on the front teeth located in the “smile zone”. These are thin ceramic plates that are fixed over the teeth and allow you to camouflage the part restored with a filling.
Dental restoration: prices in Moscow clinics (estimated cost)
| Clinic | Light-composite filling | Metal-ceramic crown | Restoration with anchor/fiberglass pin |
| City dentistry "Dento-El" | 42 USD | 135-595 USD | 9/45 USD |
| Dental clinic "Lancet" | 50-63 USD | 152-724 USD | 100/549 USD |
| "Dental Medical Center" | 23 USD | 142-156 USD | 12/67 USD |
| "KSK-Dent" | 31-76 USD | 122-155 USD | 15/23 USD |
| "Zub.ru" | 64-110 USD | 186-335 USD | 140/275 USD |
| "LeaderStom" | 28-41 USD | 54-158 USD | 26-118 USD |
Questions to check knowledge on the topic of the lesson
1. Etiology of complete destruction of the tooth crown. Clinical variants of the gingival part of the roots.
2. Classification of pin structures.
3. Requirements for the tooth root.
4. Indications for choosing a pin design depending on clinical condition gingival part of the root.
Complete destruction of the tooth crown. Etiology.
Complete destruction of the tooth crown The vast majority occurs as a result of caries, less often due to injury. The development of secondary caries due to insufficient and clinically unjustified treatment of the cavity at the initial visit, the use of low-quality material leads to chipping
And splits of tooth crowns, significant or complete loss of the crown are caused by pathological abrasion, dysplasia and hereditary disorders of dental development.
Complete defects of the coronal part of the forelock include destruction with an index of destruction of the occlusal surface of the tooth (IROPD)>0.7. In these cases, the remains of the crown part of the tooth protrude above the gum level by 2-3 mm. With such destruction, the neurovascular bundle of the pulp is, as a rule, completely necrotic, and peri-apical processes are detected. For hypoplasia
And pathological abrasion, with the most significant loss of hard tissue, the vital activity of the pulp can be preserved, in addition, there may be no pathological processes in the periapical tissues. Complete defects of the coronal part of the tooth include:
1. the presence of the gingival part of the tooth crown protruding above the level of the gingival margin by a distance of up to 3 mm;
2. the presence of hard tooth tissues at the level of the gingival margin;
3. destruction of the hard tissues of the tooth below the level of the gingival margin up to a quarter of the length of the root (with greater destruction, removal of the tooth root is indicated).
Destruction of the tooth crown leads to morphological changes dentition: nearby standing teeth tilt (converge), the antagonizing tooth moves towards the defect. The absence of the crown part of several teeth, especially adjacent ones, can lead to deformation of the dentition, bite, and dysfunction masticatory muscles and TMJ.
Types of orthopedic pin structures.
A pin tooth is fixed prosthesis, which completely replaces the tooth crown and is strengthened in the root canal with a pin.
They are distinguished depending on their purpose, design, manufacturing method and the material from which they are made. Pin structures that serve only to replace the crowns of natural teeth are called restorative.
By design, pin teeth are divided into monolithic and combined.
According to the manufacturing method - cast and soldered.
According to the material from which they are made - metal, plastic, porcelain and lined.
The metal and non-metallic parts of a pin tooth can be connected using cement (Davis, Duval crown), solder (Akhmetov pin tooth), or directly (plastic pin teeth). In some post tooth designs, a porcelain facet veneer is connected to a metal backplate by means of clasps or other devices.
L.V. Ilyina-Markosyan divides pinned teeth depending on the principle of strengthening them at the root.
In some cases, the pin tooth is adjacent with its crown part or root protective plate to the outer surface of the prepared root (plastic pin teeth), in others, the protruding part of the tooth root is covered with a ring (Richmond pin tooth), in others, the fixing part of the pin tooth is adjacent not only to the outer surface of the root, but also to the inner walls of the canal mouth (pin tooth according to Ilina-Markosyan).
1. Pin structures in which the root part is only
comes into contact with the tooth stump:
a) plastic pin tooth; b) standard pin designs (Logan, Davis, Duval, Bonneville, Forster, Steele); c) soldered pin tooth.
The disadvantage of these structures is the access of oral fluid into the root canal due to the lack of tightness.
2. Pin teeth, during the manufacture of which the mouth of the root canal is hermetically sealed with an inlay:
a) according to Ilina-Markosyan; b) according to Citrine;
c) pin stump insert.
3. Pin structures that hermetically close the tooth stump not only with a root plate, but also with an additional ring or semi-ring:
a) according to Richmond;
b) according to Katz; c) according to Akhmetov.
Classification of modern pin structures:
1. Pin structures used for urgent care, both temporary and permanent restoration crown part of the tooth (plastic pin tooth, pin tooth according to Shirakaya, etc.).
2. Universal, individually manufactured solid-cast pin structures (stump pin crown according to Kopeikin, stump pin tooth, composite stump pin inlays).
3. Industrially manufactured pins and stump inlays ( RADIXANKER, CYTCO, MOOSER, IKADENT, C-POST, etc.)
4. Composite stump inlays reinforced with polymer fibers
(“Ribbond”, etc.)
5. Pin structures for the treatment of root fractures (cast stump pin inlay with an intra-stump canal and a threaded pin by Bragina E.A. et al., intraradicular pins and an apical titanium inlay by Griban A.M. et al.)
6. Transdental pins (endodontic-endosseous implants) and parapulpal pins.
By design, pin teeth are distinguished:
1. According to Logan - a monolithic porcelain tooth connected directly to the pin.
2. According to Richmond, a supra-root protection with a ring serves as a support.
3. According to V.N. Kopeikin - a stamped steel cap as a supra-root protection and a pin fitted along the root canal.
4. According to L.V. Ilyina-Markosyan - the supporting part is in the form of a cast insert (shock absorber).
5. According to A.A. Akhmedov - a metal crown with a plastic lining and a pin.
6. According to A.Ya. Katsu - supra-root protection and half-ring.
7. According to N.A. The beam-pin tooth consists of a metal half-cap with an open vestibular surface, an elastic pin and a plastic lining.
8. According to ORTON - solid cast with a supporting insert.
9. According to Davis, it is a composite crown, consisting of a separate porcelain crown and a pin, which are connected with cement.
10. Field. Shargorodsky - the supra-root protective plate is modeled on a wax model after fitting the ring and pin along the root canal. The root protection is not stamped, it is cast together with the pin and ring.
11. According to Duvel - diatoric porcelain teeth into which pins with a special washer are attached.
12. According to V.N. Parshina - a metal ring, a pin and a polished standard tooth made of plastic;
13. According to 3.P. Shirakoy - fitted standard plastic tooth and pin. The root canal orifices are used to form the retainer tab. The pin and tooth are welded with quick-hardening plastic
Question 3.
Indications for the selection of pinned teeth designs
determined based on the following clinical situations:
1. the degree of preservation of the supragingival part of the tooth crown and the level of destruction of root tissue in relation to the gingival margin;
2. group affiliation of tooth roots - single or multi-rooted teeth;
3. the nature of the occlusal relationships - bite.
Selection of pin tooth design depends on the size of the preserved supragingival part of the tooth root, the type of bite and other conditions. Thus, with a deep bite, only solid pin teeth with plastic or ceramic lining can be used to restore the front teeth. In cases where part of the front teeth protrudes above the gum 1-2 mm (type I), pin teeth are shown according to Richmond, Katz, Shargorodsky, Akhmedov, Ilyina-Markosyan, Davis, Logan, orstump pin tab according to Kopeikin,and in the group of lateral teeth - only a stump pin crown according to Kopeikin or a stump pin tooth. For type II roots, pin teeth can be used according to Ilyina-Markosyan, Citrine, Orton, Logan, Davis, Kopeikin, plastic pin tooth.
For types III and IV roots, a stump pin inlay according to Kopeikin is indicated; in addition, restoration of the coronal part of such teeth can be done using anchor pins, followed by covering with solid crowns.
Indications for the use of pin structures:
1. Pin teeth are used to restore the crown part of a tooth in case of its complete absence or significant destruction ( index of destruction of the occlusal surface of the tooth 0.8 or more).
2. As a support for a bridge.
3. Pin structures in combination with other elements for
4. For reinforcement of pulpless teeth.
5. Pins for replanted teeth.
Contraindications to the use of pin structures:
1. Undocked pathological changes in periapical tissues.
2. Obstruction of root canals.
3. Short roots with thin walls.
4. Atrophy bone tissue alveolar process at the root by 3/4 or more.
5. Destruction of the root by more than 1/4 of its length.
6. A defect in any of the root walls is equal to or greater than 1/4 of the root size.
IN blocks combining a large group of teeth, as well as for clasp fixation, it is not recommended to use roots with significant cystic changes periapical tissues, even with successful treatment.
If the supragingival part of the tooth crown, protruding above the gingival margin, is preserved, it is possible to use all types of pinned teeth. In cases of destruction of this part of the crowns and the location of the root tissues at the gum level, it is possible to use Kopeikin pin teeth designs or solid-cast structures. The same structures are indicated for subgingival destruction of root tissue.
An important indicator of pin structures is the ratio of the length of the pin and the vertical size of the coronal part. The length of the pin inserted into
root canal, corresponds to half or more of the length of the root and cannot be less than the vertical dimension of the restored coronal part.
For pins, standard clasps and orthodontic wire of various diameters should be used, corresponding to the diameter of the root canal. The shape of the pin is rectangular, oval.
The choice of a pin structure depends on the condition of the root and the qualifications of the doctor. The main attachment between the root and the extra-root part of such a prosthesis is a pin, which transmits pressure to the root walls, so there are
general clinical and technical rules for the tooth root:
The root must stand above the gum or be at the same level with it (this requirement is relative, since in other cases a different design should be chosen);
the root must be stable in the hole;
there should not be any in the area of the root apex inflammatory changes in periodontal tissues;
the root walls must be of sufficient thickness and should not be affected by caries or other pathological process;
the root canal must be passable to a length no less than the height of the crown;
the root canal cannot be curved over two thirds of its length, counting from the enamel-cement junction;
the circular ligament of the tooth should not be damaged;
the root canal must be obturated with filling material to at least one third from the apical foramen.
Requirements for the roots of teeth serving as support for post structures:
1. The root canal must be well passable over a length equal to the length of the pin.
2. The near-apical part of the root canal should be well sealed and the apical periodontium should be free of signs of acute or chronic inflammation ( granuloma, cystogranuloma, cyst, etc.). In the presence of periapical changes, if they are not extensive, in the absence of fistulas and good filling At the root apex, prosthetics with a pin tooth is permissible. If there is significant periodontal damage to the root apex, prosthetics with a pin tooth can be performed after root resection, if sufficient root length remains.
3. The root must be longer than the height of the future crown.
4. The walls must be of sufficient thickness (at least 2 mm) to withstand the chewing pressure transmitted through the pin, and
speaking | affected | caries. |
5. The root stump should be open. If it is covered by the gum, then a gingivectomy is performed.
6. The root must be stable.
Based on the clinical condition of the supra-alveolar part, 4 types of roots can be distinguished, which can be used as a support when restoring the coronal part of the teeth (F.N. Tsukanova, 1986):
Type I - roots with preserved supragingival part (2 mm or more);
Type II - roots at the gum level with preservation of the walls;
Type III - roots whose edges are hidden under the gum;
Type IV - roots with destruction of the bifurcation.
The absence of conditions is a contraindication for the manufacture of pin structures. The nature of the bite should be taken into account, i.e. with a deep bite, preliminary orthodontic treatment is necessary, and if there are defects in the lateral parts of the dentition, their replacement is necessary. It is also necessary to take into account the anatomical, topographical and age characteristics root canal.
^ LDS. Complete absence (destruction) of the tooth crown
1. Pin teeth, in | 2. Pin teeth, | 3. Pin teeth, |
|
Types of pins | of which the root | hermetically sealed |
|
designs | part is in contact with | in which the mouth | covering the stump |
tooth stump (Logan, | root canal | not only teeth |
|
closes with a tab | supraroot |
||
(according to Citrine, | record, but also |
||
Ilyina-Markosyan) | ring (by |
||
Richmond, Akhmetov) |
|||
^ Requirements, | |||
presented | must be on | the tooth is on | must perform |
gum level and be | gum level and | above the gum by 1.5-2 |
|
sealed until | sealed until | mm and be |
|
tops | tops | sealed until |
|
tops |
|||
Indications | Complete destruction | ||
upper teeth crowns | |||
for use | |||
pin | |||
designs | |||
Deep bite | |||
Contraindications | length mismatch | ||
root crown |
Characteristic various types pin structures. Pin tooth with ring according to Richmond. Currently
used extremely rarely. This design consists of a ring, a supra-root protective plate and a pin. It can be made if the crown part protrudes above the gum by 2-3 mm. Measure the root circumference with a thin wire or dentimeter. According to this length, a ring is made from 900 gold alloy, 0.25-0.28 mm thick, 4-4.5 mm high, to which a plate is soldered to form a cap. After fitting the cap on the root, a hole is made in the plate through which a gold-platinum alloy pin is fitted, an impression is taken, a model is obtained in which the pin is connected to the cap with gold solder, and again it is applied to the stump. Complete impressions are taken from the dentition of both jaws, and the models are plastered in an occluder. The future metal bed for the facet is modeled from wax, cast and soldered to the cap. Then a porcelain facet is ground and attached to the cap and metal stock or a plastic lining is made. After this, the pin tooth is adjusted and strengthened with cement.

Due to the complexity of manufacturing a soldered cap, a design with a stamped steel cap has become widespread - the Richmond pin tooth in the MMSI modification. The protective cap is the main advantage of the Richmond pin tooth design: the ring provides reliable protection the part of the root protruding above the gum from the ingress of saliva, the development of caries and decementation.
Positive qualities:
- Possibility of use with thin walls of the tooth root, strengthens them with a ring;
- the cap prevents saliva from entering and decementing the pin structure;
- can be used as a support for a bridge.
Negative qualities:
Translucent metal in the neck of the tooth, plastic quickly changes color.
Stages of manufacturing a pin tooth according to Richmond: 1. - preparation of the root;
2. - obtaining the dimensions of the root circumference;
3. - fitting of the ring and pin;
4. - obtaining an impression with a ring and a pin and making a model;
5. - fitting the mouthguard with a pin;
6. - taking impressions and casting a model with a mouth guard;
7. - making a crown;
8. - fixation of the prosthesis in the oral cavity.
The tooth is prepared so that the root protrudes 1.5 mm above the gum level. To measure the circumference of the root, use a loop of wire with a diameter of 0.4 mm (bindrat), remove the loop from the root, cut it, straighten the wire and cut a strip of the required length and width along its length from a gold plate (900 standard). Using pliers, a ring is made from the strip, the edges of which are placed end-to-end, soldered with 750-grade solder and fitted to the root. The edges are contoured along the neck of the tooth and moved under the gum by 0.5 mm. To obtain a mouthguard, a gold plate and a gold pin are soldered to the ring. Impressions are then taken and the models with the mouthguard are cast. They are cast into an occluder and a crown of the design chosen by the doctor is made.
Pin tooth according to Akhmedov. The root of the tooth is prepared in compliance with the rules for preparing the tooth for a full metal crown. The tooth stump serves as a support for a tight fit of the edge of the crown and must protrude above the level of the gum. After fitting the metal crown, the oral wall of the crown is perforated with a bur in accordance with the projection of the root canal, and a previously fitted stainless wire pin is inserted through the hole into the root canal. An impression with a pin is obtained and the color of the plastic is determined. In the laboratory, a model is obtained, a pin is soldered to the crown and a window is cut out on its vestibular surface. After veneering, a crown is fitted with a pin in the mouth.
Stages of manufacturing a pin tooth according to A.A. Akhmedov.
This design is especially convenient when the gingival part of the crown is preserved.
1. preparation of the coronal part of the tooth
2. taking impressions of both dentitions
3. production of stamped crowns;
4. fitting the pin and crown in the clinic;
5. obtaining an impression and determining the color of the future plastic cladding;
6. soldering of teeth and pins in the laboratory, manufacturing of veneers;
7. grinding, polishing;
8. The finished tooth with a pin is placed in the oral cavity and fixed with cement.
Lesson No. 14
Lesson topic: Complete absence (destruction) of the tooth crown. Etiology. Clinical and radiological assessment of the tooth root. Pin teeth, their classification, conditions and indications for prosthetics with various designs. Formation of root canals for the pin.
Purpose of the lesson: Disassemble the classification of pin structures.
To study the indications for the use of pinned teeth depending on the clinical condition of the gingival part of the root. Study the principles of forming root canals under a pin.
Questions to check the initial level of knowledge
Anatomical features of the structure of the teeth of the upper and lower jaw.
X-ray examination of the roots used for pin structures.
1. WIDTH OF THE PERIODONTAL FIGURE IN THE MIDDLE THIRD OF THE ROOT
RAVNA (A.S.SHCHERBAKOV)
0.1-0.12 mm, 3) 0.16-0.19 mm,
2. THE WIDTH OF THE PERIODONTAL FIGURE IN THE APOPHICAL THIRD OF THE ROOT IS EQUAL (A.S.SHCHERBAKOV)
0.1-0.12 mm, 3) 0.16-0.19 mm,
0.08-0.14 mm, 4) 0.23-0.27 mm.
3. FUNCTIONING TEETH HAVE A PERIODONTAL GAP COMPARED TO TEETH OUT OF FUNCTION
4. PHYSIOLOGICAL TEETH MOBILITY IS ON AVERAGE
0.01-0.03 mm, 3) 0.1-0.5 mm,
0.05-0.1 mm, 4) about 1 mm.
Standards of answers to control tasks of the initial level of knowledge.
– 2; 2) – 3; 3) – 2; 4) – 1.
Summary of training material
Complete destruction of the tooth crown The vast majority occurs as a result of caries, less often due to injury. The development of secondary caries due to insufficient and clinically unjustified treatment of the cavity at the initial visit, the use of low-quality material leads to chipping and splitting of the crowns of the teeth. Pathological abrasion, dysplasia and hereditary disorders of tooth development lead to significant or complete loss of the crown. Complete defects of the coronal part of the tooth include destruction with an index of destruction of the occlusal surface of the tooth (IROPD) of 0.7. in these cases, the remains of the crown part of the tooth protrude above the gum level by 2-3 mm. With such destruction, the neurovascular bundle of the pulp is, as a rule, completely necrotic, and peri-apical processes are detected. In case of hypoplasia and pathological abrasion, with the most significant loss of hard tissues, the vital activity of the pulp can be preserved, in addition, there may be no pathological processes in the periapical tissues. Complete defects of the coronal part of the tooth include:
the presence of the gingival part of the tooth crown protruding above the level of the gingival margin at a distance of up to 3 mm;
the presence of hard dental tissues at the level of the gingival margin;
destruction of hard tooth tissues below the level of the gingival margin up to a quarter of the root length (with greater destruction, removal of the tooth root is indicated).
Destruction of the tooth crown leads to morphological changes in the dentition: adjacent teeth tilt (converge), the antagonizing tooth shifts towards the defect. The absence of the crown part of several teeth, especially adjacent ones, can lead to deformation of the dentition, bite, dysfunction of the masticatory muscles and the temporomandibular joint.
Pin teeth are distinguished depending on their purpose, design, manufacturing method and the material from which they are made. Pin structures that serve only to replace the crowns of natural teeth are called restorative. By design, pin teeth are divided into monolithic and combined. According to the manufacturing method - cast and soldered. According to the material from which they are made -
for metal, plastic, porcelain and lined.
The metal and non-metallic parts of a pin tooth can be connected using cement (Davis, Duval crown), solder (Akhmetov pin tooth), or directly (plastic pin teeth). In some post tooth designs, a porcelain facet veneer is connected to a metal backplate by means of clasps or other devices.
L.V. Ilyina-Markosyan divides pinned teeth depending on the principle of strengthening them at the root. In some cases, the pin tooth is adjacent with its crown part or root protection plate to the outer surface of the prepared root (plastic pin teeth), in others, the protruding part of the tooth root is covered with a ring (Richmond pin tooth), in others, the fixing part of the pin tooth is adjacent not only to the outer surface of the root, but also to the inner walls of the canal mouth (pin tooth according to Ilina-Markosyan).
Pin structures in which the supra-root part only comes into contact with the tooth stump:
a) plastic pin tooth;
b) standard pin designs (Logan, Davis, Duval, Bonneville, Forster, Steele);
c) soldered pin tooth.
The disadvantage of these structures is the access of oral fluid into the root canal due to the lack of tightness.
Pin teeth, during the manufacture of which the mouth of the root canal is hermetically sealed with an inlay:
a) according to Ilina-Markosyan;
b) according to Citrine;
c) pin stump insert.
Pin structures that hermetically close the tooth stump not only with a root plate, but also with an additional ring or semi-ring:
a) according to Richmond;
b) according to Katz;
c) according to Akhmetov.
The choice of a pin structure depends on the condition of the root and the qualifications of the doctor. The main attachment between the root and the extra-root part of such a prosthesis is a pin, which transmits pressure to the root walls, so there are
general clinical and technical rules for tooth roots :
The root must stand above the gum or be at the same level with it (this requirement is relative, since in other cases a different design should be chosen);
The root must be stable in the hole;
In the area of the root apex there should be no inflammatory changes in the periodontal tissues;
The root walls must be of sufficient thickness and should not be affected by caries or other pathological process;
The root canal cannot be curved over two thirds of its length, starting from the enamel-cement junction;
The circular ligament of the tooth must not be damaged;
The root canal must be obturated with filling material to at least one third from the apical foramen.
The absence of conditions is a contraindication for the manufacture of pin structures. The nature of the bite should be taken into account, i.e. with a deep bite, preliminary orthodontic treatment is necessary, and if there are defects in the lateral parts of the dentition, their replacement is necessary.
It is also necessary to take into account the anatomical, topographical and age-related features of the equine canal.
Indications for choosing a pinned teeth design determined based on the following clinical situations:
the degree of preservation of the supragingival part of the tooth crown and the level of destruction of root tissue in relation to the gingival margin;
group affiliation of tooth roots - single or multi-rooted teeth;
the nature of the occlusal relationships - bite.
If the supragingival part of the tooth crown, protruding above the gingival margin, is preserved, it is possible to use all types of pinned teeth. In cases of destruction of this part of the crowns and the location of the root tissues at the gum level, it is possible to use Kopeikin pin teeth designs or solid-cast structures. The same structures are indicated for subgingival destruction of root tissue.
An important indicator of pin structures is the ratio of the length of the pin and the vertical size of the coronal part. The length of the pin inserted into the root canal corresponds to half or more of the length of the root and may be less than the vertical dimension of the restored coronal part.
For pins, standard clasps and orthodontic wire of various diameters should be used, corresponding to the diameter of the root canal. The shape of the pin is rectangular, oval.
The process of preparing the tooth root is determined by the design of the prosthesis and consists of a number of stages: elimination of the source of inflammation, if any, expansion of the root canal, filling of the canal, preparation of the canal for insertion of the pin, preparation of the root stump. By removing necrotic tissue, an appropriate surface is created, which provides a support for the base of the pin tooth.
In the vast majority of cases, complete loss of the crown occurs as a result of caries, less often due to injury; Pathological abrasion, dysplasia and other hereditary disorders of dental development lead to significant or complete destruction of the tooth crown.
A special group consists of destruction of the crown part of the tooth after caries treatment. The development of secondary caries after filling necessitates repeated treatment of hard tissues, which leads to an increase in the volume of the cavity in the tooth and thinning of the hard tissues of the crown (Fig. 81). Secondary caries develops as a result of insufficient and clinically unjustified treatment of the cavity during initial treatment, the use of low-quality material and in cases where an inlay is indicated. The same reasons lead to chipping and splitting of tooth crowns.
Complete defects of the coronal part of the tooth include destruction with IROP > 0.7. In these cases, the remains of the crown part of the tooth protrude above the gum level by 2-3 mm. As a rule, the neurovascular bundle of the pulp is completely necrotic and periapical processes are detected. In case of hypoplasia and pathological abrasion, even with a significant loss of hard tissues, up to the level of the gums, the vital activity of the pulp and the absence of pathological processes in periapical tissues.
Complete defects of the crown part of the tooth include: 1) the presence of the gingival part of the tooth crown protruding above the level of the gingival margin up to 3 mm (more preservation of 1 - 2 walls is possible); 2) the presence of hard tooth tissues at the level of the gingival margin; 3) destruction of hard tooth tissues to the level of root tissues and below the level of the gingival margin within up to a quarter of the root length (with greater destruction, tooth root removal is indicated).
In the situations specified in paragraphs 2 and 3, the marginal periodontium is inflamed, partially hypertrophied and can overlap the remaining hard tissues root However, this is not an indication for tooth root removal, since hypertrophied tissue can be excised or coagulated using an electrocoagulator. This approach to preserving tooth roots and restoring the crown of a tooth with the listed degrees of destruction is justified by the preventive focus of the domestic orthopedic school.
Destruction of hard tissues chewing teeth is the primary trigger for the occurrence of diseases of the dental system. The destruction of the occlusal and contact surfaces causes the development of macromorphological shifts in the structure of the dentition: changes in the size of segments of chewing teeth, deformation of the occlusal surface, the disappearance of characteristic closure areas on the occlusal surface of antagonizing teeth, which together represents a manifestation initial symptoms functional disorganization. A further increase in destruction of the occlusal surface is associated with an increase in tension (tension) of the tooth walls, which, under the influence of chewing load, are responsible for their destruction up to total loss crowns The involvement of several chewing teeth in this process leads in the border zones to a decrease in the content of the mineral and protein components of the jaw bones in the area of the teeth that are excluded from function; pronounced histomorphological restructuring of periodontal tissues, disruption of the structure of the dentition and functional interaction antagonizing teeth.
Complete defects of the coronal part of a number of teeth determine the qualitative uniqueness of the function of the dental system, namely the function of chewing. Zones with increased functional load and non-functioning zones are identified, where general patterns of the emergence and development of pathological processes characteristic of both hyperfunction and hypokinesia appear. Possible oppression metabolic processes in the jaw bones, the phenomena of atrophy, dystrophy and inflammation of periodontal tissue. The destruction of the crowns of -2 teeth does not cause a significant impairment in the function of biting and chewing food, it is painless and practically asymptomatic. In such cases, deformation of the dentition and bite, the development of periodontal diseases occur slowly and, therefore, become important early diagnosis developing negative restructuring of the dental system and knowledge of pathogenesis possible complications after tooth extraction, which determine the indications for preventive orthopedic treatment.
The absence of the crown part of several teeth, especially adjacent ones, can lead to deformation of the dentition, bite, dentoperiodontal tissue failure, dysfunction of the masticatory muscles and temporomandibular joints, similar to those with the loss of similar teeth. In the overwhelming majority of cases, people with a destroyed crown part of a tooth are asked to remove this “tooth.” If a doctor removes the root of a tooth without assessing the complex of indications for removal, he makes a grave mistake.
At the current level of development of the specialty, using a complex treatment method (physiotherapeutic, therapeutic), it is possible and should preserve almost all tooth roots.
The destruction of the crown part of the tooth should be regarded as a disease leading over time to pathological condition or disease of organs and the entire dental system.
It is not difficult to determine the complete absence of the crown part of a tooth. However, it is necessary to carry out additional examination to identify possible complications in the periapical tissues and in the entire dental system. At complete destruction The following complications are possible in the crown of a tooth (they must be included in the diagnosis): necrosis of pulp tissue; periodontitis - acute or chronic (the latter is distinguished between fibrous, granulating, granulomatous-granuloma).
The loss of the crown part of a tooth (teeth) can lead to significant changes in the morphological structure of the dentition (see Chapter 5): 1) adjacent teeth, due to the disappearance of contact points, tilt (converge) in the direction of the defect; 2) the antagonizing tooth(s) shifts towards the dentition defect.
These changes exacerbate clinical picture underlying disease and complicate the diagnosis. It is possible, for example, like this clinical case with a diagnosis of “complete destruction of the coronal part of the first molar of the lower jaw, convergence of the second premolar and second molar; complete destruction of the coronal part of the first molar of the lower jaw, supraocclusal displacement of the first molar of the upper jaw.”
Developing complications caused by the destruction of the crown of the tooth change medical tactics.
Basics of restorative orthopedic interventions.
The starting point of orthopedic interventions in case of complete destruction of the tooth crown is a position in which, after restoration of the coronal part, the tooth is fully connected to the chewing function. Restoring the crown part of a tooth is prophylactic. Underestimation of the preventive significance of restoring the crown part of the tooth in the presence of the root(s) of the tooth in everyday practice leads to unnecessary root removal. Removal of a tooth or its roots causes inevitable resorption of interdental septa and a decrease in the functionality of the periodontium of adjacent teeth.
Before deciding on root removal, the feasibility of preserving and restoring the tooth should be analyzed in order to prevent the development of further destruction of the dental system; the condition of the peri-apical tissues and the possibility of stopping pathological processes in them; the possibility of using the root as a future fulcrum for the prosthesis.
In this regard, restoration of the coronal part in the presence of tooth roots in the oral cavity is possible: 1) with completely stopped processes in the periapical tissues. This means that the root canal of the tooth is filled with complete obturation of the hole in the apex of the tooth or with the filling material extending beyond the apex. In cases of minor or complete obstruction of the root canals, the root cannot be removed (analogue - a tooth with chronic periodontitis), since treatment methods such as ionogalvanization, silver plating, resorcinol-formalin are possible. Treatment in this situation is carried out after creating artificial canals in the roots of the teeth (according to the projection of natural ones) to accommodate the pin. Resorption of the walls of the alveoli in the root area should not exceed half the length of the root; 2) with a root wall thickness of 1 mm for the anterior teeth of the lower jaw and at least 2 mm for the remaining teeth. A vertical defect in any of the root walls is no more than a quarter of the root size. The initial indicators for determining this type of damage are the level of the non-inflamed gingival margin and radiographic data.
Tooth roots must be removed for the following reasons:
1) the presence of common chronic diseases unknown etiology;
2) if preserving the roots does not improve the conditions for prosthetics;
3) the presence of significant changes in the periapical tissues and the impossibility of stopping the pathological process;
4) grade III and IV bone tissue atrophy;
5) destruction of the root by more than a quarter of its length.
The main thing when diagnosing complete destruction of the crown of a tooth and the presence of its root is the postulate that there is no difference in the indications for the removal of teeth that have retained the coronal part or the root of the tooth, i.e., a tooth that has lost the coronal part. This position is based on the fact that the periodontium of each tooth functions regardless of the presence of a natural or artificial tooth crown.
Treatment in the absence of a tooth crown is carried out using pin teeth.
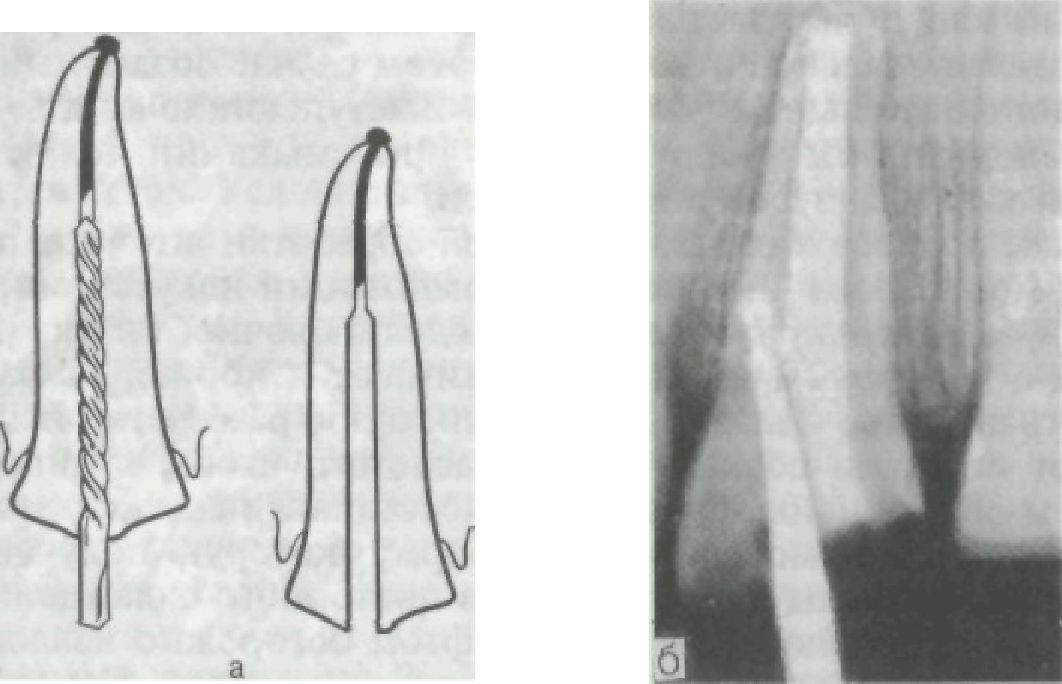
A pin tooth is a permanent prosthesis used to restore the destroyed crown and partly the root part of the tooth (Fig. 82). It consists of an artificial crown or a stump covered with an artificial crown and a post. The latter is inserted into the canal of the preserved tooth root. It is one of the main elements of the prosthesis design, allowing it to be fixed.
Currently known large number different pin designs. Based on the manufacturing method and clinical indications, it seems appropriate to distinguish IV main groups:
1) stump crown (stump pin inlay);.
2) solid cast pin tooth;.
3) pin tooth according to Richmond;.
4) simple pin teeth.
A distinctive feature of such prostheses is the design of the crown part.
The main requirements for a pinned tooth, its quality and effectiveness are reliable isolation of the preserved root surfaces from the oral environment and strengthening it due to its tight coverage in the cervical part by the structural element. These requirements are met only by a stump pin insert with the subsequent production of an artificial crown, a solid cast (with or without lining) pin tooth; pin tooth according to Richmond in the MMSI modification.
Rice. 82. The main types of modern pinned teeth. a - stump pin insert and its varieties; b - according to Richmond; c - solid cast with lining.
Indications for the selection of pin teeth designs are determined based on the following clinical situations: 1) the degree of preservation of the supragingival part of the tooth crown and the level of destruction of root tissue in relation to the gingival margin; 2) group affiliation of the roots of the teeth - single- or multi-rooted teeth; 3) the nature of the occlusal relationships - the type of bite.
If the supragingival part of the tooth crown, protruding above the gingival margin, is preserved, it is possible to use all types of pinned teeth. In cases of destruction of this part of the crowns and the location of the root tissues at the gum level, it is possible to use pin teeth designs according to Kopeikin or solid cast structures.
The same structures are indicated for subgingival destruction of root tissue. The Richmond pin tooth and simple pin teeth are contraindicated in such clinical situations.
The Richmond pin tooth is not used when restoring crowns of multi-rooted teeth.
If there is a deep bite and there is a need to restore the crown of the front tooth, it is impossible to use stump pin structures and a Richmond pin tooth. In these cases, only solid-cast pin teeth are indicated (aesthetic veneering is determined based on specific clinical situations).
An important indicator of pin structures is the ratio of the length of the pin and the vertical size of the coronal part. The length of the pin inserted into the root canal corresponds to half the length of the root or more and cannot be less than the vertical dimension of the restored coronal part.
For pins, standard clasps and orthodontic wire of various diameters should be used, corresponding to the diameter of the root canal. Standard pins are most effective. Solid pins can be used, but they may have internal pores and are therefore less durable. When using a pin structure, this defect can lead to a fracture of the prosthesis.
The process of preparing the tooth root is determined by the design of the prosthesis and consists of a number of stages: elimination of the source of inflammation, if any, expansion of the root canal (Fig. 83), filling the canal with cement, preparing the canal for insertion of the pin, preparation of the root stump. Preparation is carried out
Rice. 83. Correct (a) and incorrect (b) position of the bur when expanding the root canal.
burs or shaped diamond heads, removing necrotic tissue and creating an appropriate surface that provides support for the base of the pin tooth.
Stump crowns.
In outpatient practice they use various options stump crowns: developed by V. N. Kopeikin, A. L. Grozovsky and Ya. B. Kovaleva. They consist of an artificial stump of the coronal part of the tooth with a pin, which is then covered with a crown with veneering, metal crown or a plastic crown. Core structures make it possible to preserve and restore most tooth roots, both single- and multi-rooted. They have a number of advantages over the design of teeth with pins. The treatment of the remaining part of the tooth crown or root surface is carried out according to the type of tooth preparation for an ordinary crown, i.e., the preserved part of the root is given the shape and diameter of the tooth neck. The bottom and remaining walls of the coronal part are processed in such a way that there are no sharp edges that could break under pressure. These tooth elements, as well as the root canal, are good retention points and contribute to the fixation of the artificial stump. The bottom of the cavity should be flat. The root walls should not be tapered at the entrance to the canal, as this will create a splitting moment on the root.
Picked up and sharpened metal pin. If a multi-rooted tooth is restored with a stump, then freely passable channel the main pin is inserted, and in difficult-to-pass areas, additional pins are inserted to a depth of 3-5 mm. If it is not possible to insert a pin into a difficult canal, the canal is widened, creating an oval hole. In this case, the created channel will be an additional fixation. The protruding ends of the pins should not be round and, when closing the jaws, should not touch the antagonist teeth.
After selecting and appropriately processing the pins, modeling of the wax composition of the artificial tooth crown begins. A stick of refractory modeling wax is softened and pressed with some force onto the root, trying not to displace the pins. After cooling the wax with water, use a slightly heated trowel to remove excess wax so that the stump has the shape and volume of the neck of the tooth. Then the chewing surface is restored, i.e., the shape that is obtained when preparing the tooth for a crown is modeled. After cooling again, the wax reproduction along with the pin is carefully removed and transferred to the laboratory for metal casting. The root canal is filled with a cotton swab and a temporary artificial dentin dressing is applied.
On the next visit to the patient, the metal stump of the tooth is fitted with a pin according to the rules for fitting the inlays. During fitting, you should ensure a tight fit of the entire cast part of the stump to the root and coronal surfaces of the tooth. The artificial tooth stump is fixed with a pin using cement.
The artificial stump of the coronal part created in this way is securely and firmly fixed to the root and can serve as a support not only for single crown, but also for other types of prostheses (Fig. 84).
If subsequently the artificial stump with a pin is covered with a plastic, porcelain, solid-cast or combined crown, then the stump is modeled in such a way as to create a ledge in the cervical part. In this case, the simulated stump is significantly smaller in size than the stump of the tooth crown after its preparation. Sometimes the stump turns into a cast root protection with a thickened supra-root part of the pin.
To reduce the number of visits, it is possible to obtain an impression after modeling the wax composition of the stump. The impression must be made with elastic masses. With this option, the technician casts a stump and makes a crown using a plaster model.
If, due to clinical conditions, it is difficult to model a stump in the oral cavity, the doctor, after fitting the pins, takes an impression of this area of the dentition. In the laboratory, a technician uses an impression to make a fire-resistant model and uses it to model the shape of the stump of the tooth to be restored. Then follows the process of converting the wax composition into metal. After casting, the stump without processing is transferred to the clinic for fitting.
IN recent years Anchor pins are also used to restore the damaged crown part of teeth.
Anchor pins are structural elements that are fixedly fixed (cemented) in the root canal of a tooth and serve for additional fixation of restoration elements. Conventionally, anchor pins consist of two parts - root and crown. The root portion may be helical or horizontal grooved for better retention. The crown part, as a rule, is an elongated rectangle, with cuts made at the corners. Using special holders fixed to these cuts, the pin is inserted into and out of the root canal. Anchor pins are made of steel, gold alloys, titanium alloys, etc.
Anchor pins come in a variety of lengths and thicknesses. They are produced in sets, the most convenient are sets with 6 length sizes, 2-3 options each cross section for each length. Some manufacturing companies offer an assortment of reamers - drills of appropriate sizes - for a set of anchor pins. This allows you to more accurately prepare the root canal for pin installation.
When installing the pin special attention is given as tight a fit as possible between the protruding, wide (coronal) part of the pin and the mouth of the root canal. It must be taken into account that the screw threads on some pins are intended only for additional retention, and not at all for screwing the pin into the canal - this can lead to splitting of the tooth root. If necessary, the pin can be adjusted to the length of the tooth root by shortening (sharpening) its intraroot cha
Minimum `/
length of the tooth root.
The anchor pin is fixed in the root canal with cement. Then, using modern composite materials and standard caps, the coronal part of the stump inlay is modeled, which is given the shape of a tooth stump prepared for an artificial crown.
Using anchor pins, you can restore both single-rooted and multi-rooted teeth. However, despite the undoubted advantages of such structures, it should be remembered that the connection of a stump made of composite material with a metal anchor pin do not provide the structural strength that solid stump inlays have.





